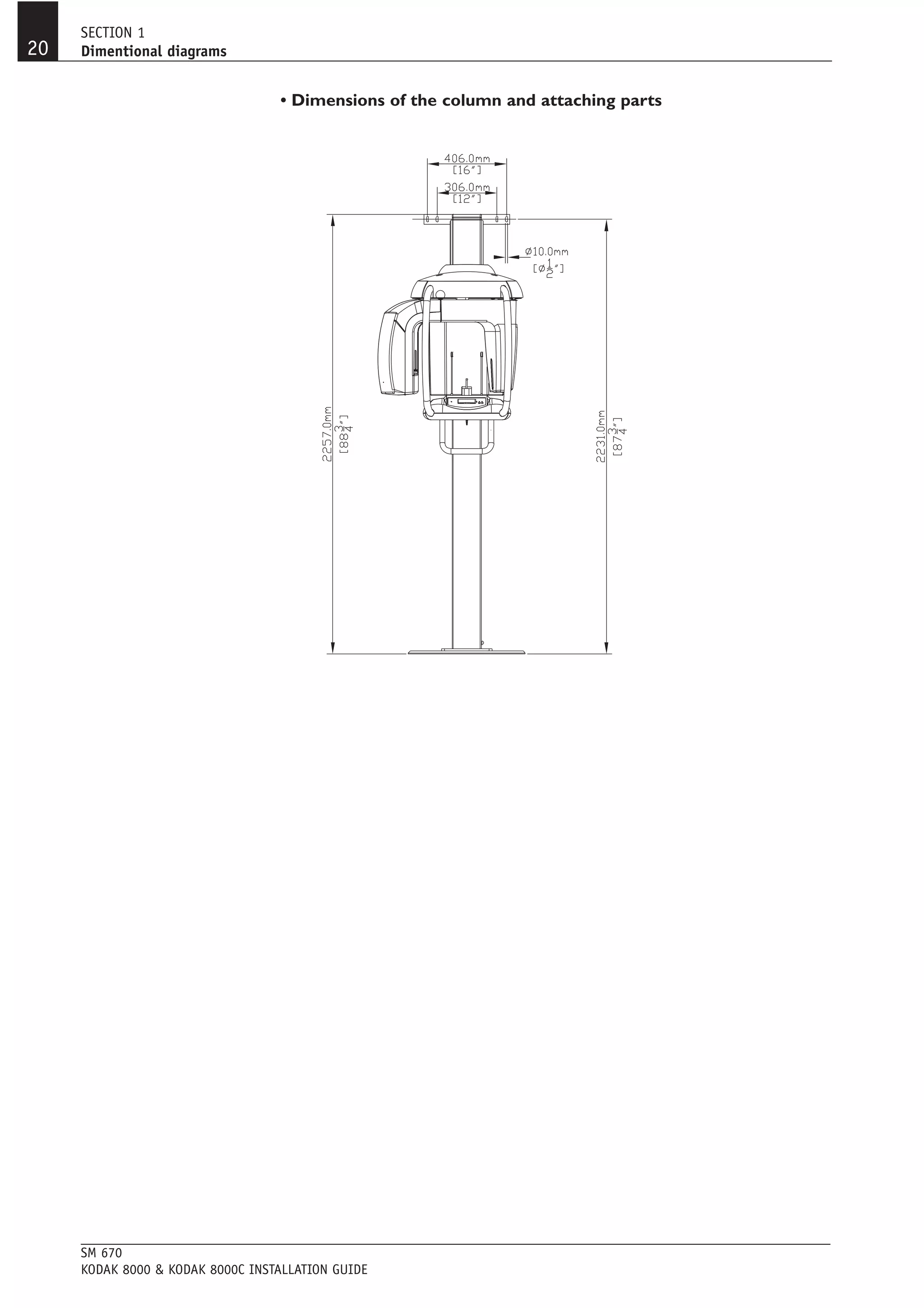
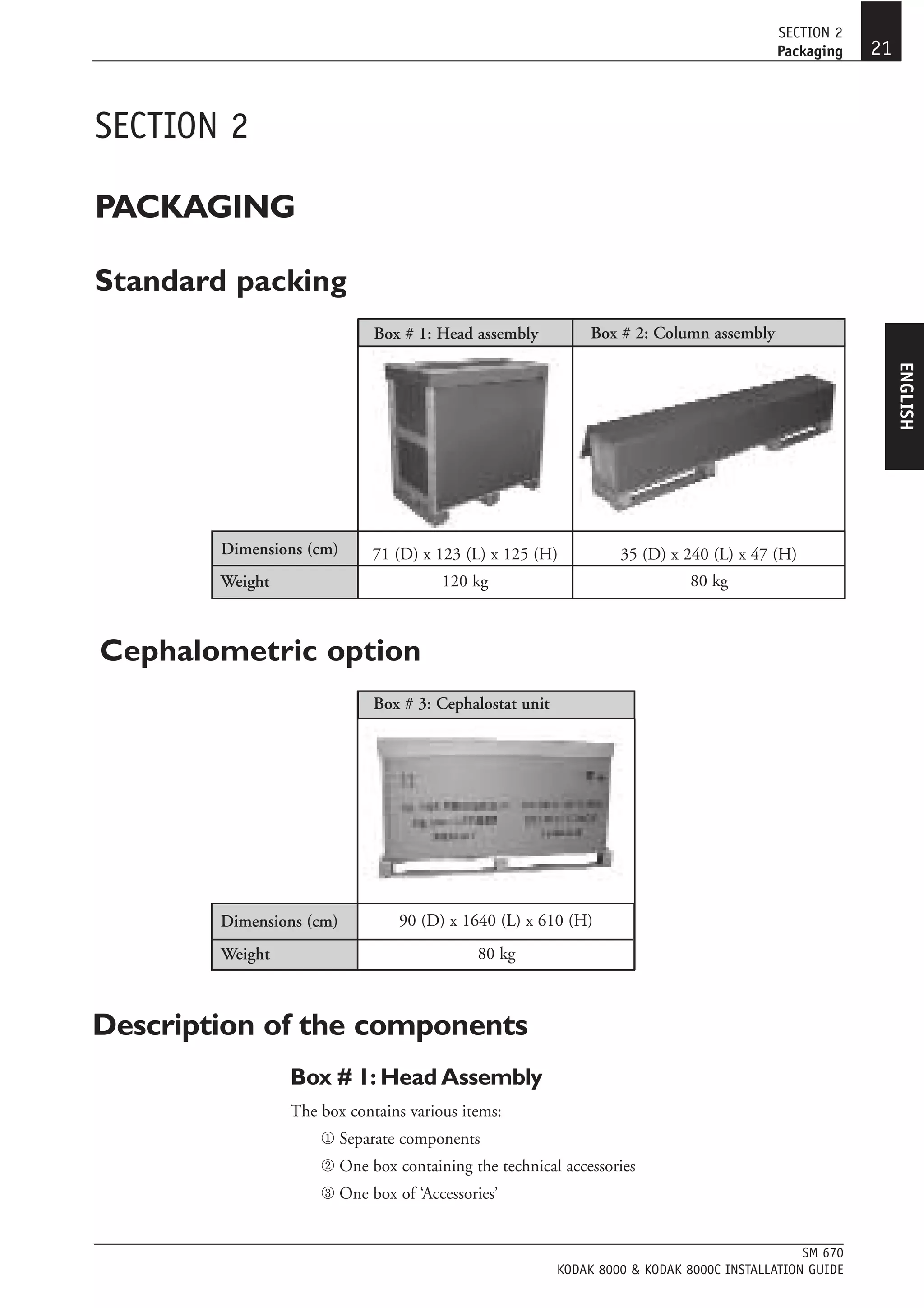
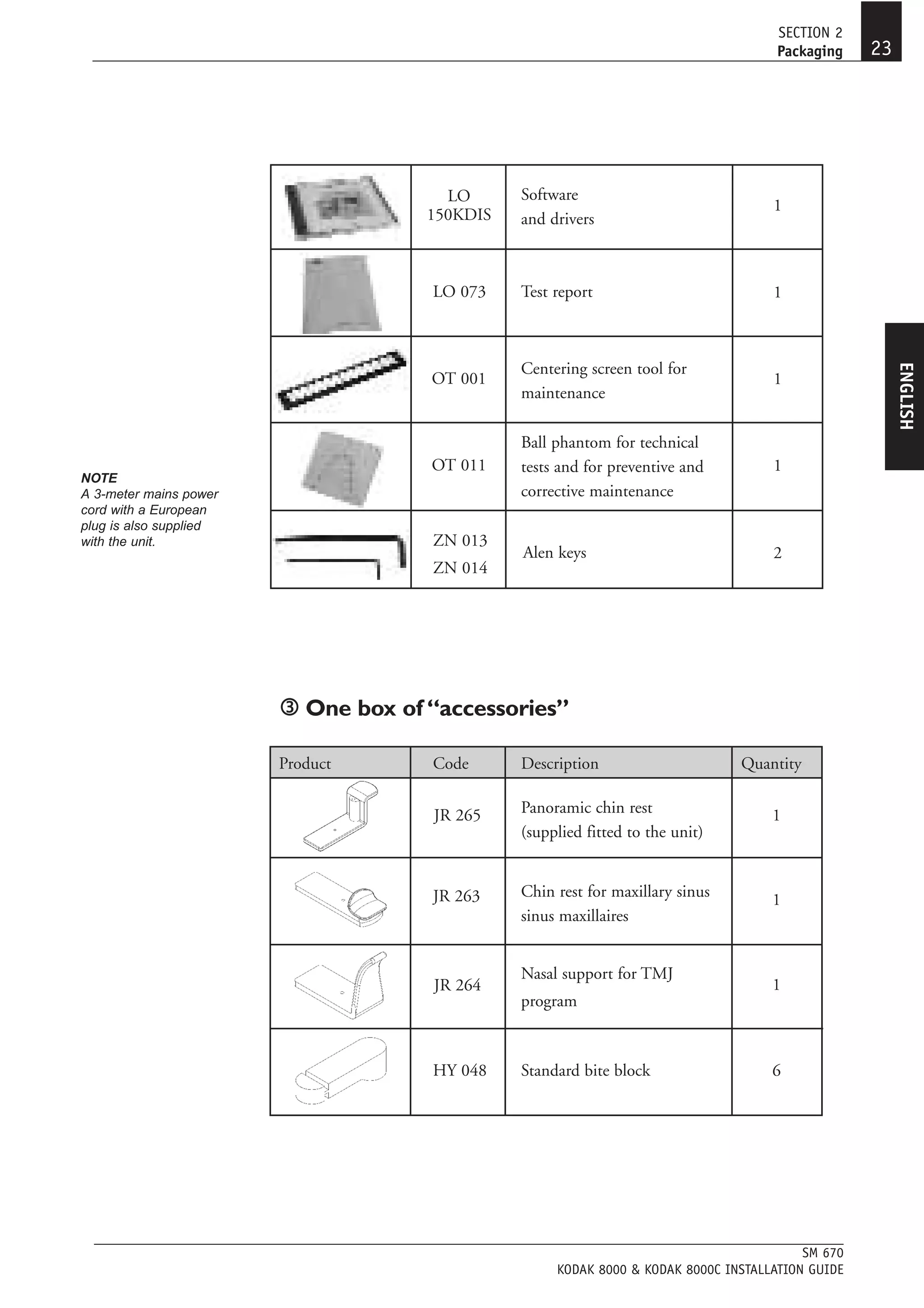
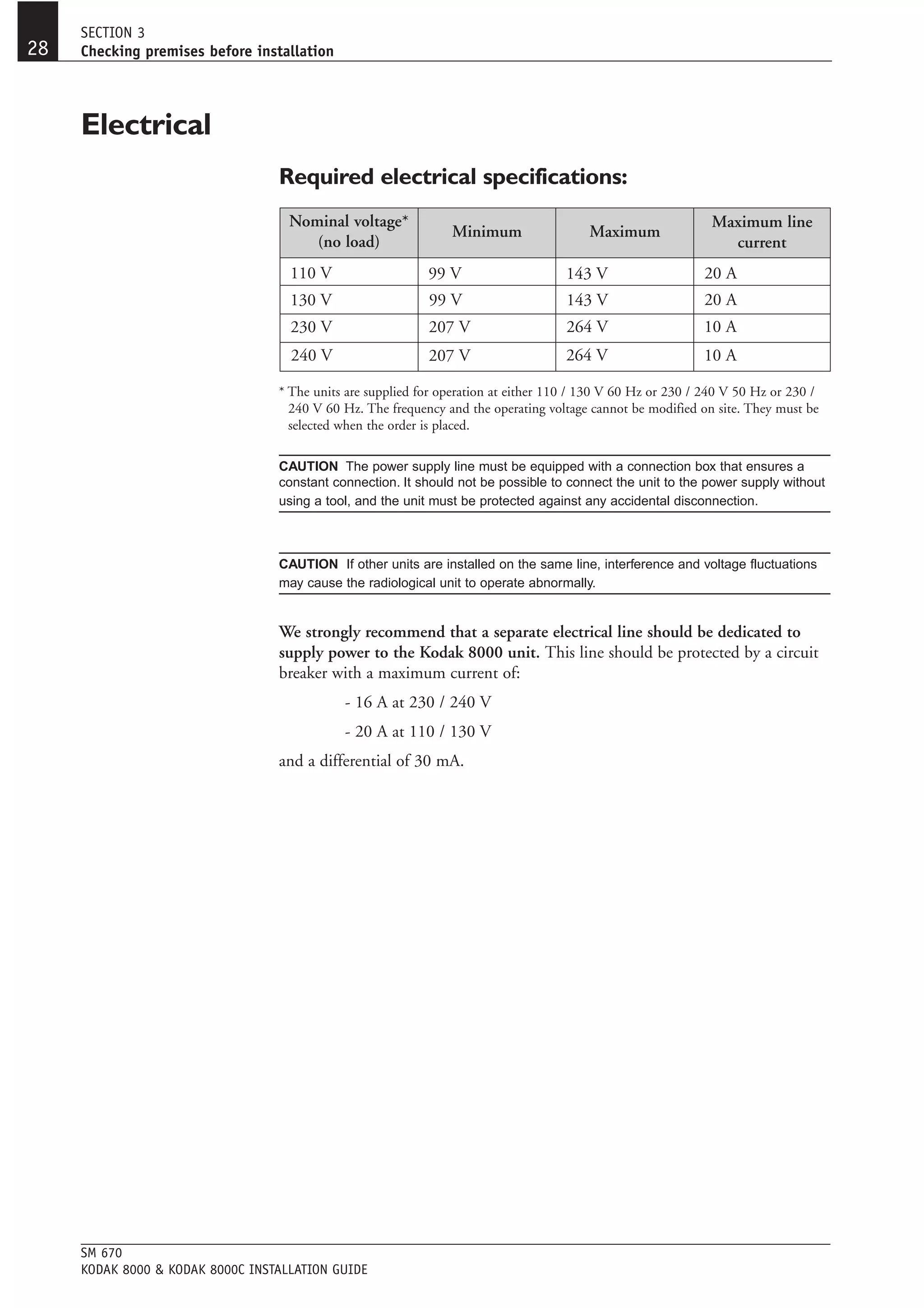
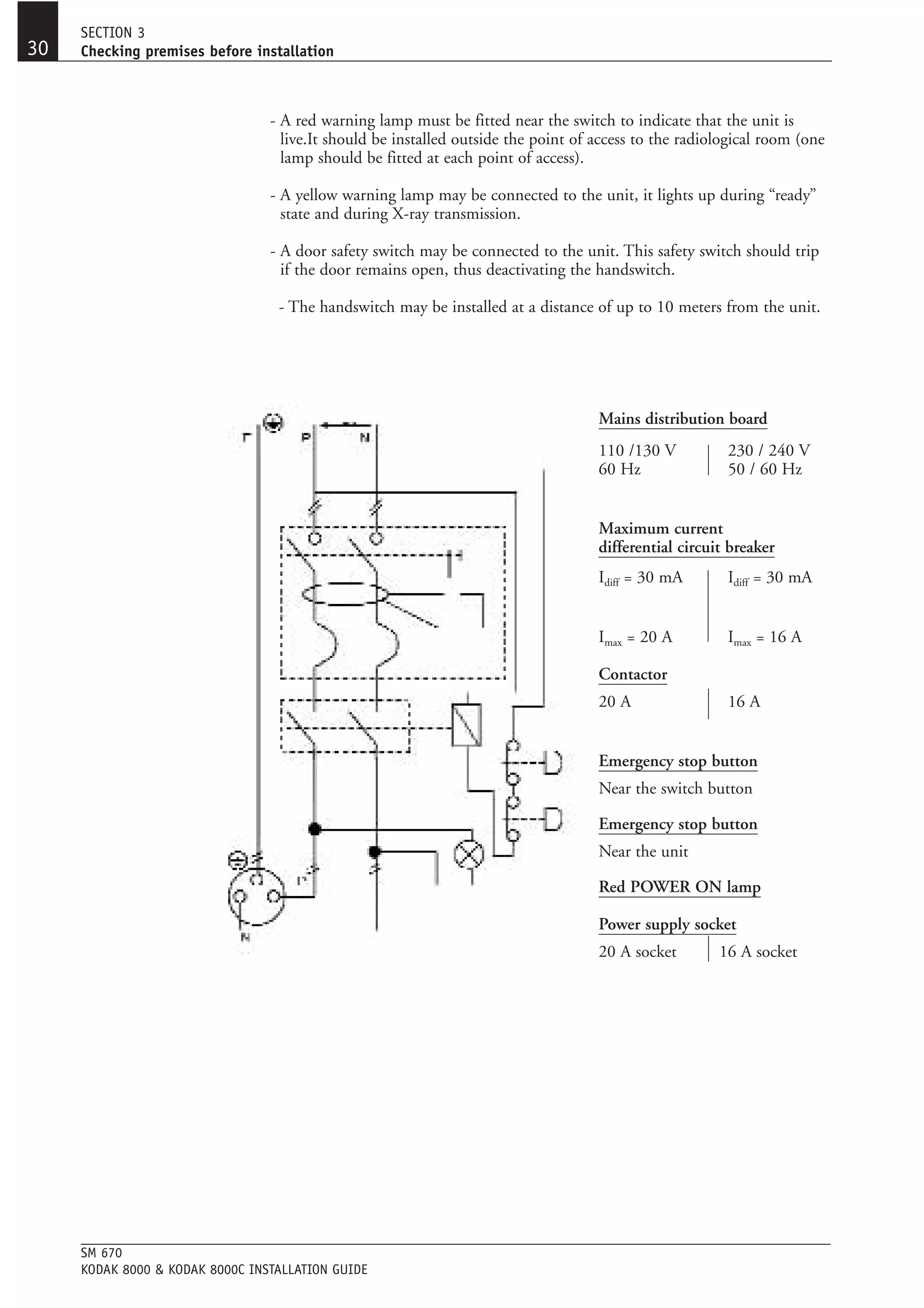
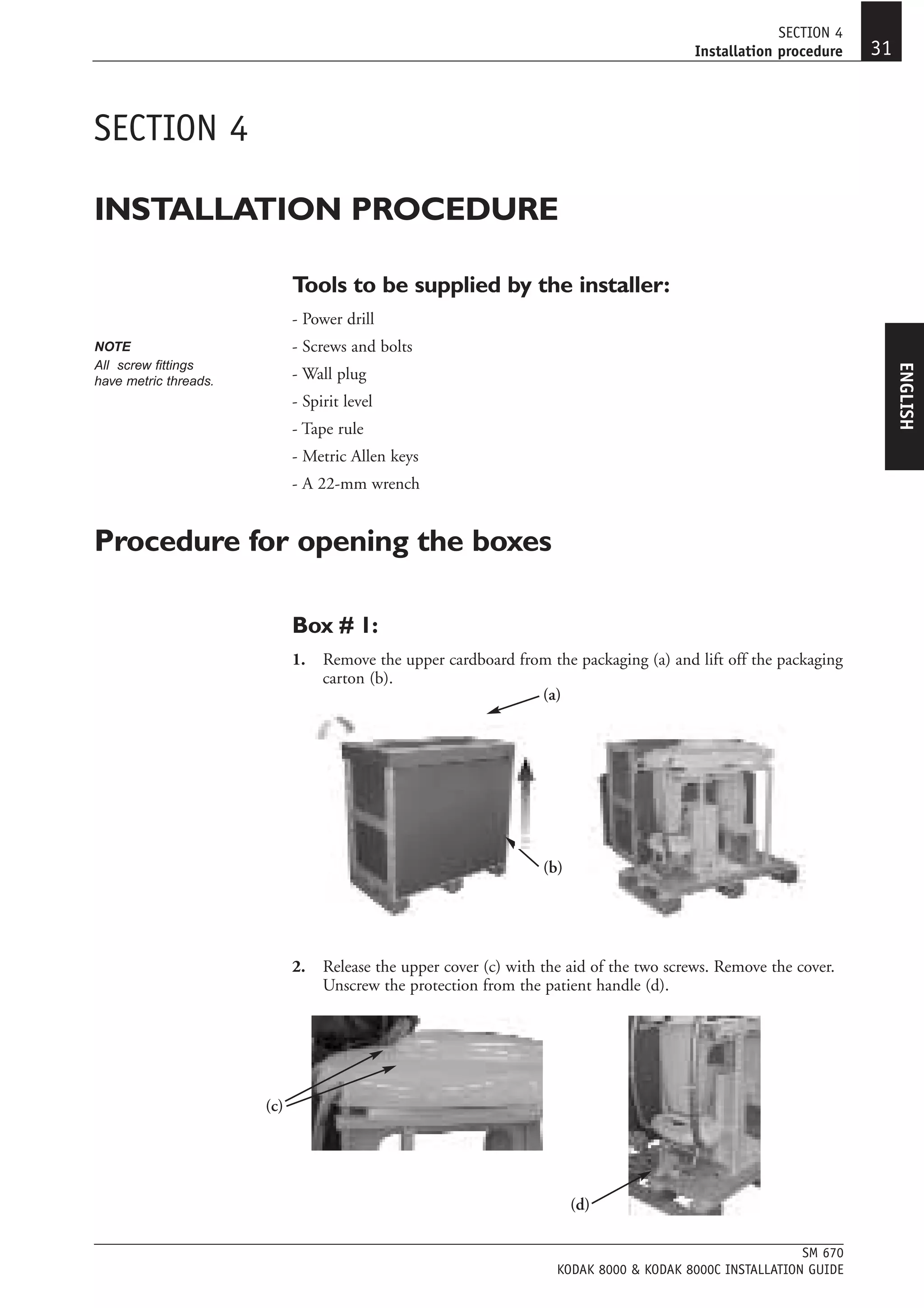
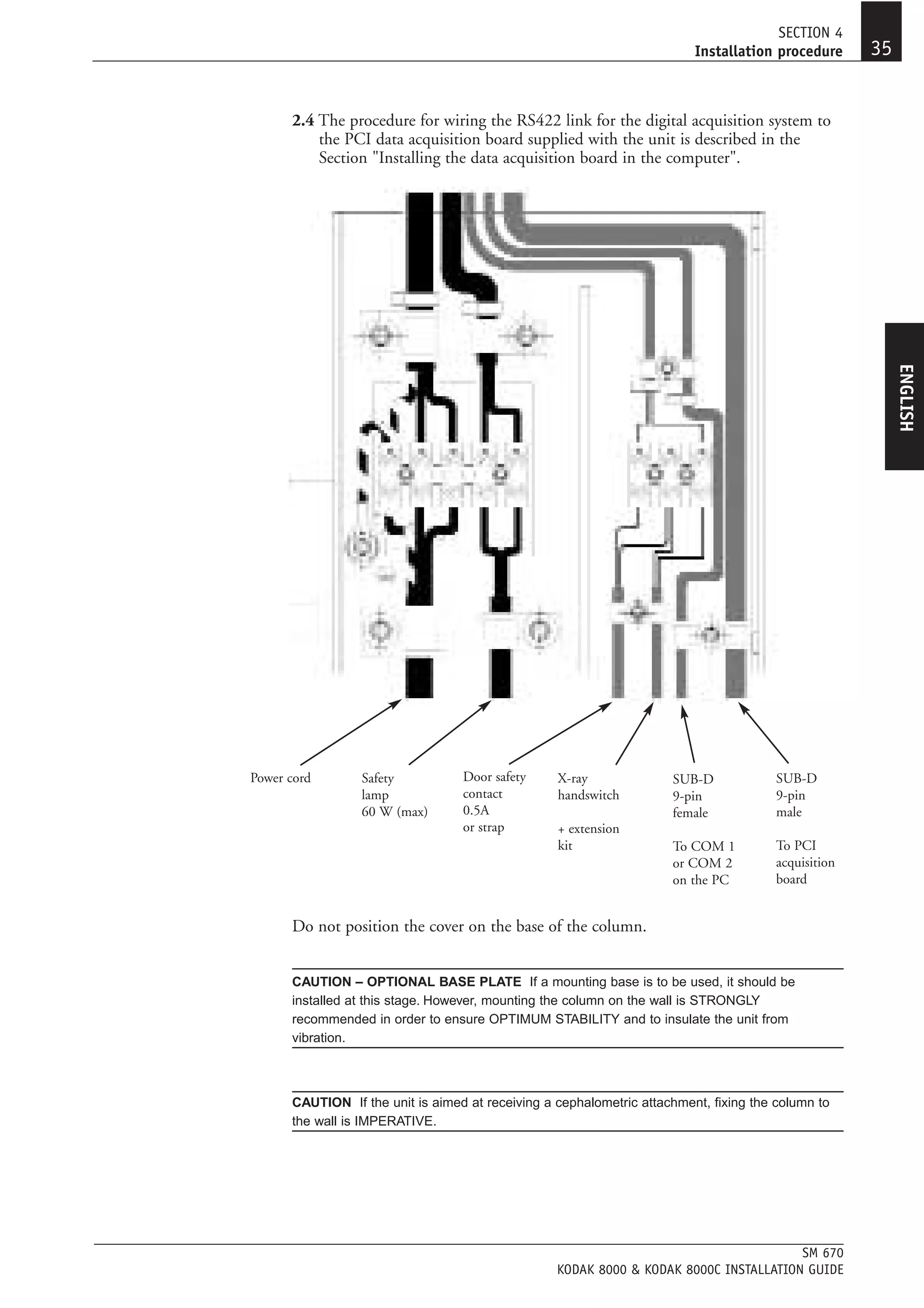
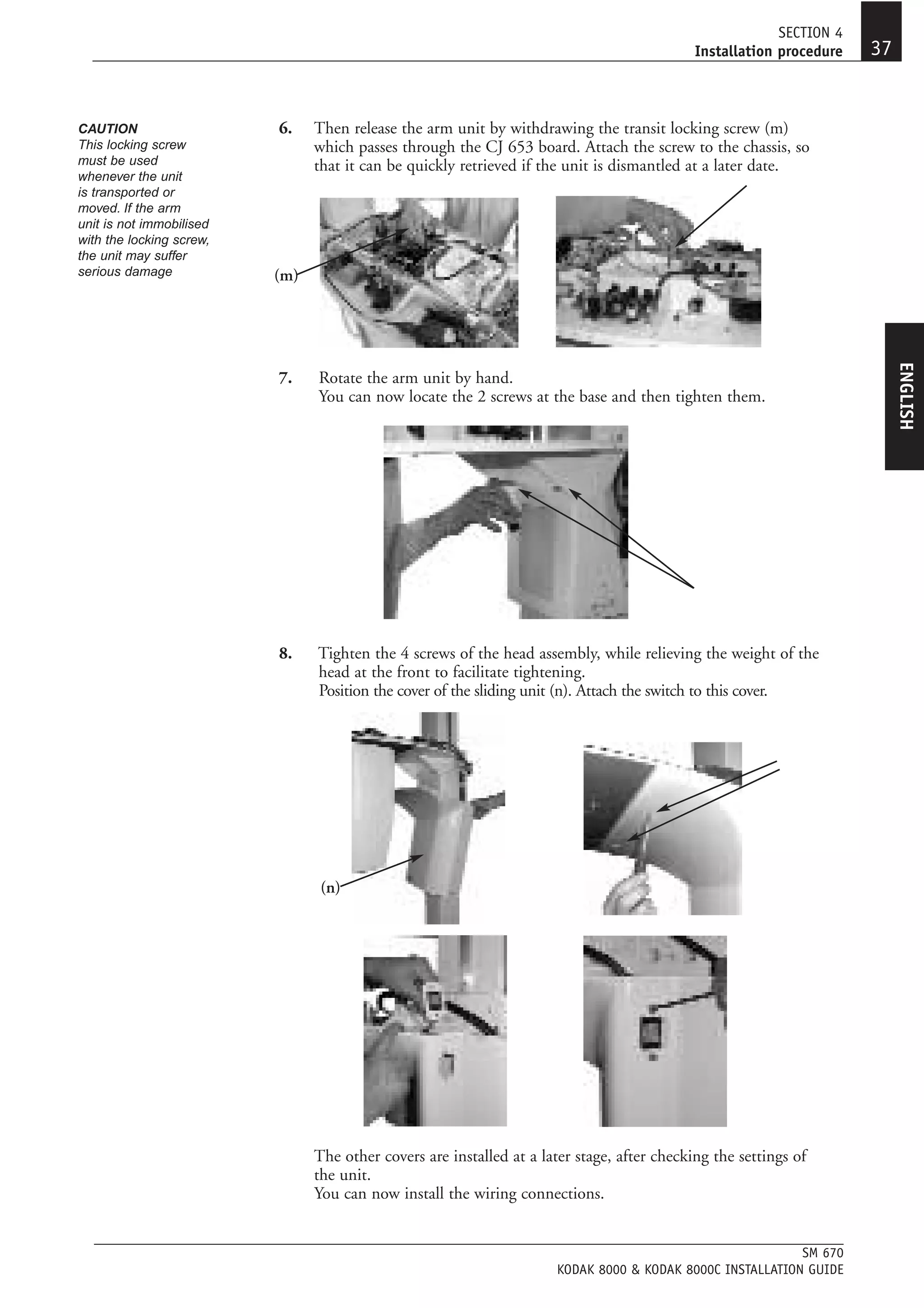
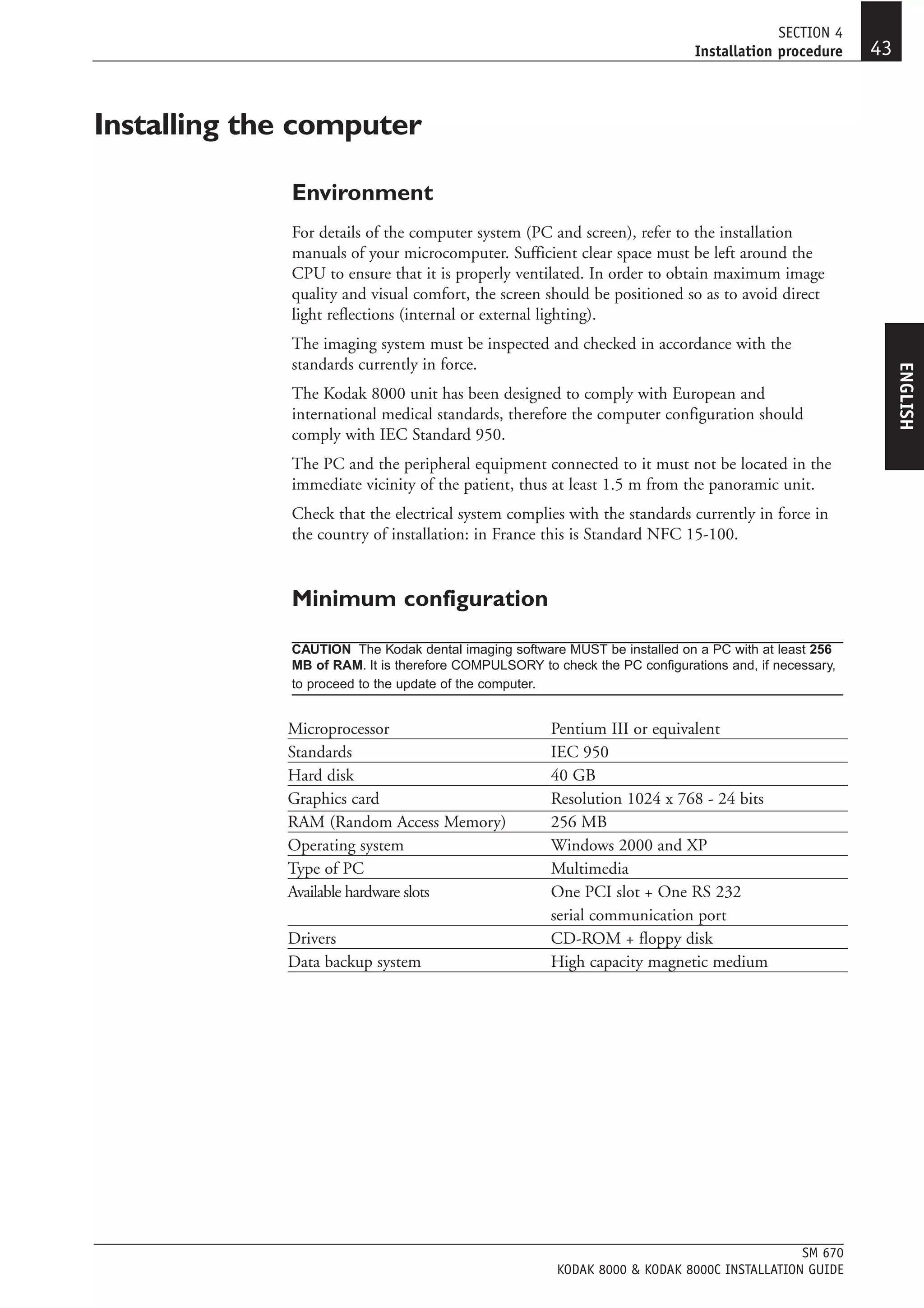
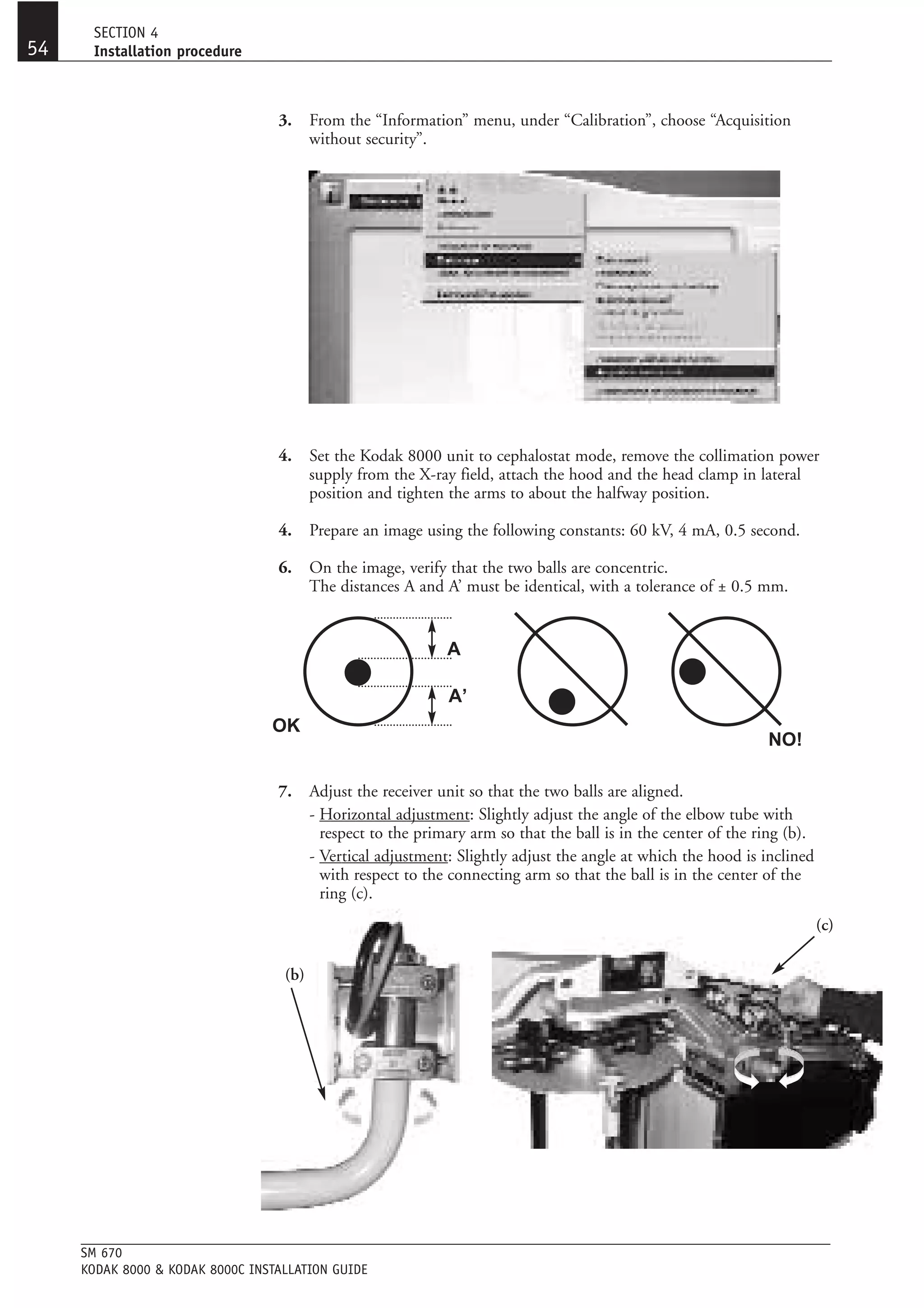
The document provides installation instructions for a Kodak 8000/8000C dental panoramic and cephalometric x-ray unit. It includes dimensional diagrams, packaging details, installation procedure steps, technical specifications, and safety and maintenance information. Installers are instructed to thoroughly read the manual in order to properly set up the unit in compliance with radiation standards and ensure safe operation.