Downloaded 50 times

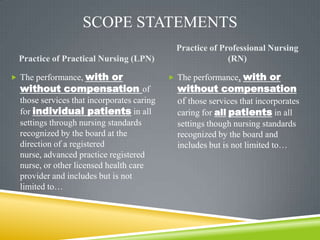




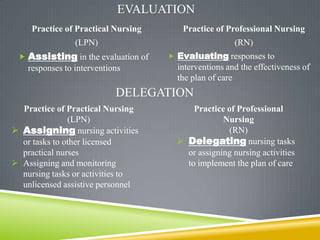









This document outlines changes to the scope of practice for licensed practical nurses (LPNs) in Minnesota based on revisions to the state's Nurse Practice Act. It summarizes the key differences between the scopes of LPNs and registered nurses (RNs), such as LPNs conducting focused assessments versus RNs providing comprehensive assessments. It also discusses implications of the changes for LPN education programs and differences in how LPNs practice in various hospital departments. Recommendations are made to better educate RNs and standardize LPN roles across units.























































































