Downloaded 15 times

![SSiiggnniiffiiccaannccee cchhaassiinngg bbiiaass
The greatest threat [to the credibility of clinical research]
may come from the poor relevance and scientific rationale
and thus low pre-study odds of success of research efforts.
Given that we currently have too many research findings,
often with low credibility, replication and rigorous evaluation
becomes as important or even more important than
discovery. Credibility, replication, and translation are all
desirable properties of research findings, but only modestly
correlated.](https://image.slidesharecdn.com/canberramostfalseactivist-140917081751-phpapp01/75/Are-most-positive-findings-in-psychology-false-or-exaggerated-An-activist-s-perspective-30-2048.jpg)
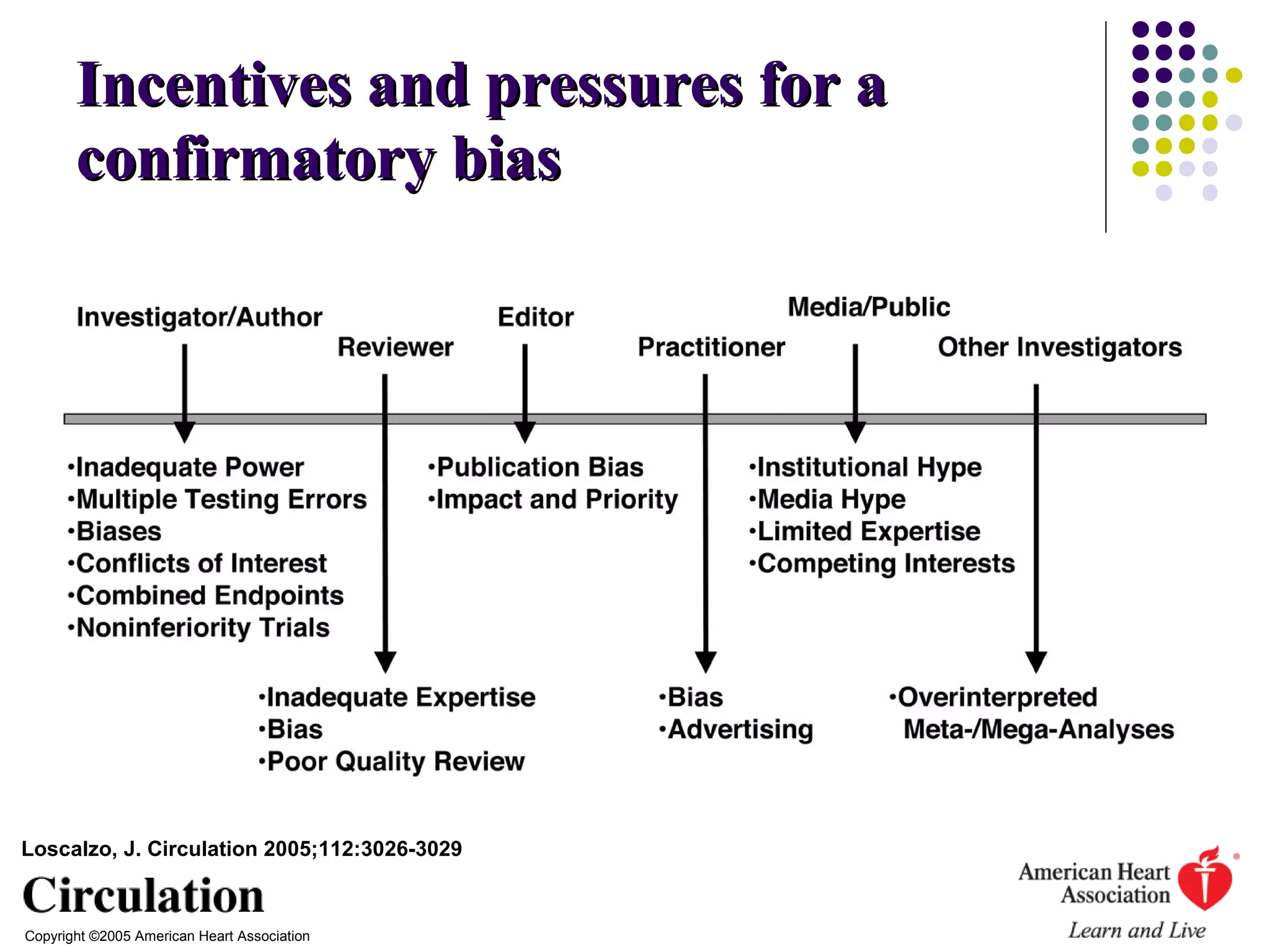






This document summarizes a presentation given by James Coyne on issues with reliability and bias in positive psychology findings. Some key points: - John Ioannidis and others have shown that many positive findings in biomedical research do not replicate and are exaggerated or false due to biases. - Similar issues exist in psychology due to confirmatory bias, flexible data analysis and chasing statistical significance. - Reforms are needed like pre-registering studies, transparent reporting standards, and making data available for independent analysis. - However, challenges remain as journals prefer positive results and organizations have conflicts of interest that uphold certain findings. Overall, skepticism is needed regarding many claimed research findings.



















![[READ]❤book⚡ Mausner & Bahn Epidemiology An Introductory Text](https://cdn.slidesharecdn.com/ss_thumbnails/0721661815-210304171858-thumbnail.jpg?width=640&height=640&fit=bounds)









![Why I Design For Human Variability [DML Conference 2016 Ignite Talk]](https://cdn.slidesharecdn.com/ss_thumbnails/rhianongutierrezdml-160916093448-thumbnail.jpg?width=640&height=640&fit=bounds)





































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






