
Recommended
Recommended
More Related Content
Similar to BUS308 Week 4 Lecture 1 Examining Relationships Expect.docx
Similar to BUS308 Week 4 Lecture 1 Examining Relationships Expect.docx (20)
More from curwenmichaela
More from curwenmichaela (20)
Recently uploaded
Recently uploaded (20)
BUS308 Week 4 Lecture 1 Examining Relationships Expect.docx
- 1. BUS308 Week 4 Lecture 1 Examining Relationships Expected Outcomes After reading this lecture, the student should be familiar with: 1. Issues around correlation 2. The basics of Correlation analysis 3. The basics of Linear Regression 4. The basics of the Multiple Regression Overview Often in our detective shows when the clues are not providing a clear answer – such as we are seeing with the apparent continuing contradiction between the compa-ratio and salary related results – we hear the line “maybe we need to look at this from a different viewpoint.” That is what we will be doing this week. Our investigation changes focus a bit this week. We started the class by finding ways to describe and summarize data sets – finding measures of the center and dispersion of the data with means, medians, standard deviations, ranges, etc. As interesting as these clues were, they did not tell us all we needed to know to solve our question about equal work for equal pay. In fact, the evidence was somewhat contradictory depending upon what
- 2. measure we focused on. In Weeks 2 and 3, we changed our focus to asking questions about differences and how important different sample outcomes were. We found that all differences were not important, and that for many relatively small result differences we could safely ignore them for decision making purposes – they were due to simple sampling (or chance) errors. We found that this idea of sampling error could extend into work and individual performance outcomes observed over time; and that over- reacting to such differences did not make much sense. Now, in our continuing efforts to detect and uncover what the data is hiding from us, we change focus again as we start to find out why something happened, what caused the data to act as it did; rather than merely what happened (describing the data as we have been doing). This week we move from examining differences to looking at relationships; that is, if some measure changes does another measure change as well? And, if so, can we use this information to make predictions and/or understand what underlies this common movement? Our tools in doing this involve correlation, the measurement of how closely two variables move together; and regression, an equation showing the impact of inputs on a final output. A regression is similar to a recipe for a cake or other food dish; take a bit of this and some of that, put them together, and we get our result. Correlation
- 3. We have seen correlations a lot, and probably have even used them (formally or informally). We know, for example, that all other things being equal; the more we eat. the more we weigh. Kids, up to the early teens, grow taller the older they get. If we consistently speed, we will get more speeding tickets than those who obey the speed limit. The more efforts we put into studying, the better grades we get. All of these are examples of correlations. Correlations exist in many forms. A somewhat specialized correlation was the Chi Square contingency test (for multi-row, multi-column tables) we looked at last week, if we find the distributions differ, then we say that the variables are related/correlated. This correlation would run from 0 (no correlation) thru positive values (the larger the value the stronger the relationship). Probably the most commonly used correlation is the Pearson Correlation Coefficient, symbolized by r. It measures the strength of the association – the extent to which measures change together – between interval or ratio level measures. Excel’s Fx Correl, and the Data Analysis Correlation both produce Pearson Correlations. Most correlations that we are familiar with show both the direction (direct or inverse) as well as the strength of the relationship, and run from -1.0 (a strong and perfect inverse
- 4. correlation) through 0 (a weak and non-existent correlation) to +1.0 (a strong an perfect direct correlation). A direct correlation is positive; that is, both variables move in the same direction, such as weight and height for kids. An inverse, or negative, correlation has variables moving in different directions. For example, the number of hours you sleep and how tired you feel; the more hours, the less tired while the fewer hours, the more tired. The strength of a correlation is shown by the value (regardless of the sign). For example, a correlation of +.78 is just as strong as a correlation of -.78; the only difference is the direction of the change. If we graphed a +.78 correlation the data points would run from the lower left to the upper right and somewhat cluster around a line we could draw thru the middle of the data points. A graph of a -.78 correlation would have the data points starting in the upper left and run down to the lower right. They would also cluster around a line. Correlations below an absolute value (when we ignore the plus or minus sign) of around .70 are generally not considered to be very strong. The reason for this is due to the coefficient of determination(CD). This equals the square of the correlation and shows the amount of shared variation between the two variables. Shared variation can be roughly considered the reason that both variables move as they do when one changes. The more the shared variation, the more one variable can be used to predict the other. If we square .70 we get .49, or about 50% of the variation being shared. Anything less is too weak of a relationship to be of much help.
- 5. Students often feel that a correlation shows a “cause-and-effect” relationship; that is, changes in one thing “cause” changes in the other variable. In some cases, this is true – height and weight for pre-teens, weight and food consumption, etc. are all examples of possible cause- and- effect relationships; but we can argue that even with these there are other variables that might interfere with the outcomes. And, in research, we cannot say that one thing causes or explains another without having a strong correlation present. However, just as our favorite detectives find what they think is a cause for someone to have committed the crime, only to find that the motive did not actually cause that person to commit the crime; a correlation does not prove cause-and- effect. An example of this is the example the author heard in a statistics class of a perfect +1.00 correlation found between the barrels of rum imported into the New England region of the United States between the years of 1790 and 1820 and the number of churches built each year. If this correlation showed a cause- and-effect relationship, what does it mean? Does rum drinking (the assumed result of importing rum) cause churches to be built? Does the building of churches cause the population to drink more rum? As tempting as each of these explanations is, neither is reasonable – there is no theory or justification to assume either is true. This is a spurious
- 6. correlation – one caused by some other, often unknown, factor. In this case, the culprit is population growth. During these years – many years before Carrie Nation’s crusade against Demon Rum – rum was the common drink for everyone. It was even served on the naval ships of most nations. And, as the population grew, so did the need for more rum. At the same time, churches in the region could only hold so many bodies (this was before mega-churches that held multiple services each Sunday); so, as the population got too large to fit into the existing churches, new ones were needed. At times, when a correlation makes no sense we can find an underlying variable fairly easily with some thought. At other times, it is harder to figure out, and some experimentation is needed. The site http://www.tylervigen.com/spurious- correlations is an interesting website devoted to spurious correlations, take a look and see if you can explain them. �� Regression Linear. Even if the correlation is spurious, we can often use the data in making predictions until we understand what the correlation is really showing us. This is what regression is all about. Earlier correlations between age, height, and even weight were mentioned. In pediatrician offices, doctors will often have charts showing typical weights and heights for children of different ages. These are the results of regressions, equations showing relationships. For example (and these values are made up for
- 7. this example), a child’s height might be his/her initial height at birth plus and average growth of 3.5 inches per year. If the average height of a newborn child is about 19 inches, then the linear regression would be: Height = 19 inches plus 3.5 inches * age in years, or in math symbols: Y = a + b*x, where y stands for height, a is the intercept or initial value at age 0 (immediate birth), b is the rate of growth per year, and x is the age in years. In both cases, we would read and interpret it the same way: the expected height of a child is 19 inches plus 3.5 inches times its age. For a 12-year old, this would be 19 + 3.5*12 = 19 + 42 = 61 inches or 5 feet 1 inch (assuming the made-up numbers are accurate). Multiple. That was an example of a linear regression having one output and a single, independent variable as an input. A multiple regression equation is quite similar but has several independent input variables. It could be considered to be similar to a recipe for a cake: http://www.tylervigen.com/spurious-correlations Cake = cake mix + 2* eggs + 1½ * cup milk + ½ * teaspoon vanilla + 2 tablespoons* butter. A regression equation, either linear or multiple, shows us how “much” each factor is used in or
- 8. influences the outcome. The math format of the multiple regression equation is quite similar to that of the linear regression, it just includes more variables: Y = a + b1*X1 + b2*X2 + b3*X3 + …; where a is the intercept value when all the inputs are 0, the various b’s are the coefficients that are multiplied by each variable value, and the x’s are the values of each input. A note on how to read the math symbols in the equations. The Y is considered the output or result, and is often called the dependent variable as its value depends on the other factors. The different b’s (b1, b2, etc.) are coefficients and read b-sub-1, b- sub-2, etc. The subscripts 1, 2, etc. are used to indicate the different coefficient values that are related to each of the input variables. The X-sub-1, X-sub-2, etc., are the different variables used to influence the output, and are called independent variables. In the recipe example, Y would be the quality of the cake, a would be the cake mix (a constant as we use all of what is in the box), the other ingredients would relate to the b*X terms. The 2*eggs would relate to b1*X1, where b1 would equal 2 and X1 stands for eggs, the second input relates to the milk, etc. Summary This week we changed our focus from examining differences to looking for relationships – do variables change in predictable ways. Correlation lets us see both the strength and the direction of change for two variables. Regression allows us to see how some variables “drive” or
- 9. explain the change in another. Pearson’s (for interval and ratio data variables) and Spearman’s (for rank ordered or ordinal data variables) are the two most commonly used correlation coefficients. Each looks at how a pair of variables moves in predictable patterns – either both increasing together or one increasing as the other decreases. The correlation ranges from - 1.00 (moving in opposite directions) to +1.00 (moving in the same direction). These are both examples of linear correlation – how closely the variables move in a straight line (if graphed). Curvilinear corrections exist but are not covered in this class. Regression equations show the relationship between independent (input) variables and a dependent (output variables). Linear regression involves a pair of variables as seen in the linear correlations. Multiple regression uses several input (independent) variables for a single output (dependent) variable. The basic form of the regression equation is the same for both linear and multiple regression equations. The only difference is in the number of inputs used. The multiple regression equation general form is: Y = Intercept + coefficient1 * variable1 + coefficient2 * variable2 + etc. or Y = A + b1*X1 + b2*X2 + …; where A is the intercept value, b is a coefficient value, and X is the name of a variable, and the subscripts identify different
- 10. variables. Summary This week we changed focus from examining differences to examining relationships – how variables might move in predictable patterns. This, we found, can be done with either correlations or regression equations. Correlations measure both the strength (the value of the correlation) and the direction (the sign) of the relationship. We looked at the Pearson Correlation (for interval and ratio level data) and the Spearman’s Rank Order Correlation (for ordinal level data). Both range from -1.00 (a perfect inverse correlation where as one value increases the other decreases) to +1.00 (a perfect direct correlation where both value increase together). A perfect correlation means the data points would fall on a straight line if graphed. One interesting characteristic of these correlations occurs when you square the values. This produces the Coefficient of Determination (CD), which gives us an estimate of how much variation is in common between the two variables. CD values of less than .50 are not particularly useful for practical purposes. Regression equations provide a formula that shows us how much influence an input variable has on the output; that is, how much the output changes for a given change in an input. Regression equations are behind such commonly used
- 11. information such as the relationship between height and weight for children that doctors use to assess our children’s development. That would be a linear regression, Weight = constant + coefficient*height in inches or Y = A + b*X, where Y stands for weight, A is the constant, b is the coefficient, and X is the height. A multiple regression is conceptually the same but has several inputs impacting a single output. If you have any questions on this material, please ask your instructor. After finishing with this lecture, please go to the first discussion for the week, and engage in a discussion with others in the class over the first couple of days before reading the second lecture. ORIGINAL ARTICLE Emotion Regulation Mediates the Relationship between a History of Child Abuse and Current PTSD/Depression Severity in Adolescent Females Sufna G. John1 & Josh M. Cisler2 & Benjamin A. Sigel1 Published online: 20 April 2017 # Springer Science+Business Media New York 2017
- 12. Abstract Although experiencing child abuse (i.e., physical abuse, sexual abuse, exposure to violence) is associated with a variety of mental health difficulties, simple exposure to abuse does not produce symptoms in every individual. The current study explored emotion regulation as a mediator in the relation- ship between a history of child abuse and symptoms of post- traumatic stress and depression. Adolescent females (ages 11– 17 years) were asked to retrospectively report on their exposure to child abuse, current symptoms of PTSD/depression, and emotion regulation abilities. Caregiver report of adolescent emotional difficulties was also obtained. Analyses revealed that child abuse-exposed females, when compared to females with- out a trauma history, had worse emotion regulation abilities and increased mental health difficulties. Moreover, emotion regula- tion significantly mediated the relationship between child abuse and all assessed mental health symptoms. These findings ex- tend previous work from adult samples, underscoring the im- portance of assessing emotion regulation abilities in abuse- exposed youth. Keywords Emotion regulation . Child abuse . PTSD . Depression . Mediation . Adolescents Introduction Child Abuse Child abuse (in this study defined as physical abuse, sexual abuse, and exposure to violence) represents a widespread pub- lic health concern. In 2013, the National Child Abuse and Neglect Data System reported 122, 159 counts of physical abuse (representing 14.1% of all maltreatment reports) and 60,956 counts of sexual abuse (representing 7.0% of all mal- treatment reports) for children ages birth through 18 years. Additionally, caregiver domestic violence was reported for
- 13. 27.4% of all victims of maltreatment (ages birth through 18 years), equivalent to 127,519 children nationally (U.S. Department of Health and Human Services 2015). Of note, these statistics likely underestimate the true prevalence, as these data only reflect instances of abuse that were reported to the authorities. Child Abuse and Associated Difficulties Experiencing child abuse is associated with an increased risk for developing mood and anxiety disorders within adulthood (Briere and Jordan 2009; Greif Green et al. 2010), as well as greater engagement in problematic behavior such as substance abuse and risky sexual behavior (Arata et al. 2005; Blumenthal et al. 2008). Adolescents who have been exposed to abuse often suffer from co-morbid conditions (i.e., depression or substance abuse), complicating the diagnostic picture, treatment considerations, and degree of functional im- pairment (Donnelly and Amaya-Jackson 2004). Given the high rate of comorbid conditions in those exposed to trauma, * Sufna G. John [email protected] 1 Department of Psychiatry, University of Arkansas for Medical Sciences, Little Rock, AR, USA 2 Department of Psychiatry, University of Wisconsin, Madison, WI, USA J Fam Viol (2017) 32:565–575 DOI 10.1007/s10896-017-9914-7 http://crossmark.crossref.org/dialog/?doi=10.1007/s10896-017- 9914-7&domain=pdf
- 14. it is important to examine transdiagnostic difficulties as poten- tial mediators. Emotion Regulation One transdiagnostic feature receiving increased attention is emotion regulation, a term which incorporates emotion under- standing, awareness, acceptance, identification, and behavioral regulation/decision-making during periods of emotional dis- tress (Gratz and Roemer 2004). Early and middle adolescence (11–14 years of age referring to early adolescence, 15–17 years of age referring to middle adolescence) represent especially important developmental periods in which to study emotion regulation, and are the focus of the present study, as they in- clude a multitude of changes in autonomy and social relation- ships that require these youth, perhaps for the first time, to develop and use emotion regulation strategies largely indepen- dent of parental guidance (American Academy of Pediatrics 2015; Larson and Richards 1991; Steinberg and Avenevoli 2000). They also represent important time periods in which to study mental health disorders, due to significant cognitive and neurodevelopmental changes (Blakemore and Choudhury 2006; Blakemore 2008), the high prevalence of mental health symptoms, and the emergence of several adult disorders within these age groups (Patton et al. 2014; Paus et al. 2008). Poor emotion regulation skills are linked to a variety of mental health symptoms and appear to represent a strong transdiagnostic correlate of mental health symptoms in adults and adolescents (Aldao et al. 2010). Good emotion regulation skills during childhood and adolescence are linked to greater peer acceptance (Kim and Cicchetti 2010), concurrent and future social competence (Spinrad et al. 2006), and lower internalizing/ externalizing pathology (Kim and Cicchetti 2010). Conversely, poor emotion regulation is documented
- 15. in individuals diagnosed with anxiety and mood disorders, eating disorders, substance abuse, and those who display ag- gression or experience peer rejection and social withdrawal (Herts et al. 2012; McLaughlin et al. 2011). The Relationship between Emotion Regulation and Child Abuse Poor emotion regulation also has been heavily examined as both a maladaptive outcome of child abuse and a risk factor for developing other mental health difficulties after abusive incidents (Kring and Werner 2004). Indeed, those who have experienced childhood abuse demonstrate difficulties in recog- nition, understanding, and acceptance of emotions, as well as overall difficulties with emotion regulation (Gratz et al. 2007; Pollak and Sinha 2002; Shipman et al. 2000). Moreover, sev- eral aspects of emotion regulation have been correlated with posttraumatic stress symptoms, including low emotional ac- ceptance and clarity and impulsive decision-making during periods of distress (Ehring and Quack 2010; Lilly and Lim 2013; Tull et al. 2007; Weiss et al. 2012). Sundermann and DePrince (2015) also found that both maltreatment character- istics (e.g., types of trauma) and difficulties with emotion reg- ulation significantly predicted posttraumatic symptoms in a community sample of adolescent females with a history of maltreatment. Despite substantive research on the relationship between child abuse and mental health symptoms, much less is known about the potential mediating role of emotion regulation in the relationship between abuse exposure and mental health symp- toms, particularly in adolescents. Results from adult samples indeed demonstrate that poor emotion regulation partially me- diates the relationship between child abuse and subsequent posttraumatic and depressive symptoms (Crow et al. 2014;
- 16. Ullman et al. 2014). Research on young adults also suggests that emotion dysregulation mediates the relationship between trauma exposure and symptoms of PTSD (Goldsmith et al. 2013) and depression (Goldsmith et al. 2013; Tull et al. 2007). Examining school-aged children, Choi and Oh (2014) found that caregiver-reported emotion regulation fully medi- ated the relationship between childhood trauma, including abuse, and emotional/behavioral symptoms. Therefore, there is foundational literature to suggest that emotion regulation mediates the relationship between child abuse exposure and emotional/behavioral difficulties in several developmental pe- riods. However, the current literature does not include a con- current examination of emotion regulation and symptoms of depression and posttraumatic stress in adolescent samples with a strong history of child abuse, nor does it consistently include information from caregivers. This latter point is espe- cially crucial, as emotion regulation difficulties may bias the way that individuals report their own symptoms, underscoring the need for collateral information. The Current Study The current study explored emotion regulation as a mediator for the relationship between child abuse severity (i.e., physical abuse, sexual abuse, and witnessing violence) and mental health symptoms (PTSD and depression) in a sample of abuse-exposed adolescent females and a healthy comparison sample of adolescent females. This study addresses several limitations in the current literature by examining important developmental periods (early and middle adolescence), utiliz- ing a sample with a high degree of trauma exposure, and including self- and caregiver-reported measures of posttrau- matic and depressive symptoms. We hypothesized that emo- tion regulation would significantly mediate the relationship between child abuse and symptoms of PTSD and depression. We further hypothesized that this relationship would also exist
- 17. for caregiver-reported mental health symptoms in their chil- dren, thus avoiding potential reporter bias. 566 J Fam Viol (2017) 32:565–575 Method Participants Participants consisted of 81 early and middle adolescent girls, aged 11–16 years, who were recruited as part of two separate neuroimaging studies (Cisler et al. 2016; Lenow et al. 2014). The rationale for this age range was to focus on the important periods of early and middle adolescence while also allowing feasibility in recruitment. Participant recruitment consisted of both community-wide general advertising (e.g., newspaper ads, flyering) as well as through networking with specific trauma-focused mental health clinics and clinicians. Interested participants first underwent a phone screening to establish probable group membership (control or abuse expo- sure), which was later confirmed through the assessment mea- sures detailed below. Inclusion criteria for control girls were as follows: age between 11 and 16 years, female sex, the absence of exposure to any measured traumatic event (both abusive and non-abusive trauma – such as experiencing a natural di- saster), and current mental health disorders. Inclusion criteria for girls with a history of child abuse was as follows: age between 11 and 16 years; female sex; and a positive history of sexual abuse, physical abuse, or witnessed violence. Psychotic disorders, developmental disorders, and MRI contraindications (e.g., internal metal objects, claustrophobia) were exclusionary for all participants. Table 1 lists demographic and clinical characteristics of the sample. All procedures performed in this study were in
- 18. accordance with the ethical standards of the Institutional Review Board (IRB) and with the 1964 Helsinki decla- ration and its later amendments or comparable ethical stan- dards. All participants and caregivers provided informed con- sent into the study. Assessments Current Mental Health Diagnoses Participants whose data are analyzed in the current study were recruited as part of two separate brain imaging research studies, and as such the structured clinical interview differed between partici- pants. Participants current mental health diagnoses were assessed with either the Mini International Neuropsychiatric Interview-Kid (MINI-Kid; n = 48) or the Kiddie Schedule for Affective Disorders and Schizophrenia (K- SADS; n = 33) (Kaufman et al. 1997; Sheehan et al. 2010). Both the MINI-Kid and K-SADS are semi-structured clinical interviews that assess most mental health disorders in childhood and adolescence and have established reliabil- ity and validity (Kaufman et al. 1997; Sheehan et al. 2010), depending on the study in which they participated. Only the adolescents, and not the caregivers, completed these struc- tured interviews. Trauma Histories Participant trauma histories were gathered with the trauma assessment sections of the National Survey of Adolescents (NSA), a structured interview used in prior epide- miological studies of child abuse and mental health functioning among adolescents (Kilpatrick et al. 2000, 2003). Both abusive and non-abusive traumas (e.g., motor vehicle accident) were assessed using this measure in order to assure that those indi- viduals in the control group had not been exposed to another type of traumatic event. Child abusive events were assessed with behaviorally-specific dichotomous questions, which in- cluded: 1) sexual abuse (i.e., anal penetration, vaginal penetra-
- 19. tion, oral sex on the perpetrator, oral sex from the perpetrator, digital penetration, fondling of the adolescent, forced fondling of the perpetrator), 2) physical abuse (i.e., attacked with a weapon; attacked with a stick, club, or bottle; attacked without a weapon; threatened with a weapon; attacked with fists), 3) severe abuse from a caregiver (i.e., beaten with fists or an object to the point where bruising or bleeding occurred), 4) witnessed violence (i.e., witnessing a violent beating at home or in com- munity). Table 2 includes a list of all questions included in this study, grouped by type of trauma. Only the adolescents, and not the caregivers, completed these trauma interviews. In line with research indicating a dose-response relation- ship between the severity of child abuse exposure and risk for subsequent mental health disorders (Cisler et al. 2011a, 2011b, 2012; Kolassa et al. 2010a, 2010b), we calculated child abuse severity as the sum of the unique categories of child abuse to which the adolescent was exposed. That is, during the NSA, participants were asked to retrospectively report on the pres- ence of 29 unique types of child abuse, and their total severity was the number of unique types of child abuse to which they answered affirmatively. This child abuse severity variable was then used in subsequent analyses testing mediation within the child abuse group. The semi-structured clinical interviews and trauma assess- ments were conducted by a trained female clinical research coordinator with several years of experience administering these interviews who was working under the supervision of a licensed clinical psychologist. Emotion Dysregulation Assessment Adolescents completed the Difficulties in Emotion Regulation Scale (DERS, Gratz and Roemer 2004), a 36 item self-report or care-giver report measure of six domains of emotion regulation: awareness of
- 20. negative emotions, emotional clarity, strategies to regulate emotions, difficulty engaging in goal directed behavior during negative emotions, nonacceptance of negative emotions, and impulse control during negative emotions. Participants indi- cate how often the items were true for them on a five-point Likert scale (‘Almost never’ to ‘Almost always’). Subsequent psychometric analyses of the DERS suggested the removal of the awareness scale, which was only comprised of reverse coded items and correlates poorly with the remaining latent J Fam Viol (2017) 32:565–575 567 factors (Bardeen et al. 2012; Fairholme et al. 2013). Accordingly, we did not use the awareness scale in the present analyses. The psychometric properties of the DERS within adolescent samples has been established (Weinberg and Klonsky 2009). Chronbach’s alpha for the remaining DERS items among this sample was .95. The total DERS score was utilized as a comprehensive measure of emotion regulation, as the individual subscales within this sample were highly correlated. Adolescent Clinical Symptom Assessment Adolescents also completed the UCLA PTSD Reaction Index – Adolescent version (Steinberg et al. 2004; 2013) and the adolescent ver- sion of the Short Mood and Feelings Questionnaire (SMFQ). The UCLA PTSD Index consists of 22 items assessing DSM- IVre-experiencing, avoidance, and hyperarousal symptoms of PTSD using a five-point Likert Scale (BNever^ to BAlmost every day^). Cronbach’s alpha for the UCLA PTSD Index among this sample was .96. For the present analyses, we used a summed PTSD symptom severity score from all DSM-IV symptom items. The SMFQ consists of 13 items assessing
- 21. depression symptoms using a three-point Likert Scale. A total depression symptom severity score was created by summing all the items. Cronbach’s alpha for the SMFQ among this sample was .94. Caregiver Clinical Symptom Assessment Caregivers addi- tionally completed the Child Behavior Checklist (Achenbach 1991), a broad measure of childhood mental health difficulties across several domains. For the purpose of the present analy- ses, we focused on total internalizing symptoms, consisting of the sum of the anxious/depressed, withdrawn/depressed, and somatic complaints subscales. Cronbach’s alpha for the CBCL Internalizing items among this sample was .93. Additional Assessments Adolescent’s verbal IQ was mea- sured using the Receptive One Word Picture Vocabulary Test administered by a female research coordinator. This measure Table 1 Demographic and clinical characteristics of the sample Abuse-exposed (n = 61) Controls (n = 20) Variable Mean (frequency) SD Mean (frequency) SD P value of group difference* Age 14.44 1.51 13.7 1.6 .06 Verbal IQ 96.05 14.81 105.7 16.4 .02 Ethnicity 46% Caucasian 80% Caucasian .053 20% African 41% African American American 10% Biracial
- 22. 3% Hispanic Current PTSD 62% 0 <.001 Total number of abusive events 5.3 4.4 0 NA Direct physical abuse 43% 0 Physical abuse from caregiver 44% 0 Sexual abuse 67% 0 Witnessed violence 88% 0 DERS nonacceptance 8.1 6.9 3.3 3.8 .006 DERS goals 11.1 5.2 6.2 5.4 <.001 DERS impulse 8.1 6.1 2.1 3.3 <.001 DERS strategies 11.0 8.3 3.0 3.1 <.001 DERS clarity 7.4 5.0 4.6 4.1 .03 DERS total 45.8 26.2 19.1 15.2 <.001 UCLA PTSD Index 26.98 19.9 .25 1.1 <.001 SMFQ 10.0 7.9 2.7 3.0 <.001 CBCL – anxious 7.4 5.9 2.1 2.4 <.001 CBCL – depressed 5.1 3.5 1.1 1.8 <.001 CBCL – somatic complaints 5.0 4.9 1.3 1.8 .002
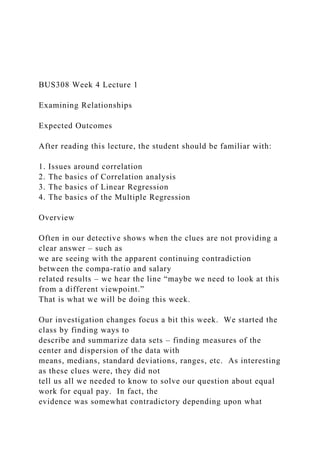
- 23. SMFQ Short Mood and Feelings Questionnaire, CBCL Child Behavior Checklist *Given evidence of group differences in age, verbal IQ, and ethnicity, the remainder of group comparisons includes these variables as covariates 568 J Fam Viol (2017) 32:565–575 was included to characterize any group differences in general cognitive function. Statistical Analyses Preliminary analyses assessed general linear model (GLM) statistical assumptions and potential confounding factors that differ between groups to be used as covariates in primary analyses. Missing data was addressed directly during data col- lection by having the research coordinator review all question- naires and if an item was missing, the participant was notified and asked to complete the item. To test hypotheses that difficulties with emotion regulation mediate the relationship between child abuse exposure and PTSD, depression, and caregiver-reported internalizing symp- tom severity, we conducted two sets of analyses to verify three predictions of a mediation pathway (Baron and Kenny 1986; MacKinnon et al. 2007; Preacher and Hayes 2008): 1) path a, such that there is a significant relation between the indepen- dent variable and the hypothesized mediator; 2) path b, such that there is a significant relation between the proposed medi- ator the dependent measure, controlling for the independent variable; and 3) that the total effect, path c (direct relation
- 24. between the independent variable and the outcome measure), weakens in the presence of the indirect effect (i.e., total effect c equals the direct effect c’ minus the indirect effect ab). Figure 1 illustrates the generic mediation framework and the hypothesized mediation pathway in the current study. First, we compared the child abuse exposed and control participants on each subscale of the DERS, adjusting for co- variates as needed, within a GLM framework using iteratively reweighted least squares estimation (‘robustfit’ in Matlab using a bisquare weighting function). These analyses effectively test path a, such that there is a relation be- tween child abuse severity and the hypothesized mediator, emotion regulation. Given that, by DSM definition, our healthy and non-trauma-exposed control group cannot have any PTSD symptoms, analyses testing paths b and the indirect effect ab were conducted solely within the child abuse group (n = 61), which required re-establishing path a within this restricted sample as well. As recommended (Baron and Kenny 1986; MacKinnon et al. 2007; Preacher and Hayes 2008), these analyses entailed four separate multiple regression GLM analyses using itera- tively reweighted least squares estimation: 1) path a, such that child abuse severity is associated with emotion regulation, 2) path b, such that emotion regulation is associated with clinical symptom severity when controlling for child abuse severity, 3) path c, such that child abuse severity is associated with clinical symptom severity, and 4) that the indirect pathway, a x b, Table 2 Trauma questions from the national survey of adolescents, organized by abuse type Physical abuse Physical abuse Witness violence Witness violence Sexual abuse
- 25. Attacked you with a gun, knife, or other weapon, regardless of when it happened or whether you told the police or other authorities? Has a caregiver ever beat you up, hit you with a fist, or kicked you hard? Heard or seen your caregivers throw objects at each other, without hitting the other person? Seen someone actually shoot someone else with a gun? Has a man or boy ever put a sexual part of his body inside your private sexual parts, inside your rear end, or inside your mouth when you didn’t want him to? Physically attacked you without a weapon, and you thought they were trying to kill or seriously injure you? Has a caregiver ever grabbed you around the neck or
- 26. choked you? Heard or seen them (caregivers) throw ob- jects that hit one an- other? Seen someone actually cut or stab someone else with a knife or other sharp weapon? Has anyone, male or female, ever put fingers or objects inside your private sexual parts or inside your rear end when you didn’t want them to? Threatened you with a gun or knife, but didn’t actually shoot or cut you? Has a caregiver ever burned or scalded you on purpose? Heard or seen them (caregivers) pushing or shoving each other? Seen someone being molested, sexually assaulted or raped? Has anyone, male or female, ever put their mouth on your private sexual
- 27. parts when you didn’t want them to? Beat you up, attacked you, or hit you with something like a stick, club, or bottle so hard that you were hurt pretty badly? Has a caregiver ever locked you in a closet, tied you up, or tied you to something? Heard or seen them (caregivers) hitting each other or beating each other up with their hands or fists? Seen someone being mugged or robbed? Has anyone, male or female, ever touched any of your private sexual parts when you didn’t want them to? Beat you up with their fists so hard that you were hurt pretty badly? Has a caregiver ever threatened you with a gun, knife, or other weapon? Heard or seen them (caregivers) hitting or
- 28. beating each other with objects, like stick, belt? Seen someone threaten someone else with a knife, a gun, or some other weapon? Has anyone, male or female, ever made you touch their private parts when you didn’t want to? Has a caregiver ever spanked or hit you so hard it caused bad marks, bruises, cuts, or welts? Has a caregiver ever used a knife or fired a gun at you on purpose? Heard or seen them (caregivers) using a weapon, like a gun or knife on each other? Seen someone beaten up, hit, punched, or kicked such that they were hurt pretty badly? J Fam Viol (2017) 32:565–575 569
- 29. significantly differs from 0 (i.e., that the difference between path c and c’ is significant). We tested the indirect ab pathway using the percentile bootstrapping method (Preacher and Hayes 2008), implemented in Matlab with 10,000 iterations and resampling with replacement. These analyses were con- ducted separately for each of the three outcome measures (PTSD symptom severity, depression symptom severity, and CBCL internalizing symptoms). Results Participant Characteristics and Preliminary Analyses Preliminary analyses indicated non-normal distributions for internalizing symptoms, child abuse severity, PTSD symptom severity, depression severity, and DERS total and subscale scores, which were corrected through square root transforma- tions in all cases except child abuse severity, which was corrected through log transformation. Participant characteris- tics are provided in Table 1. As can be seen, the child abuse and control groups differed either significantly or marginally significantly in terms of age, IQ, and ethnicity; thus, these variables were include as covariates in all subsequent analy- ses. Adolescent girls who had experienced child abuse dem- onstrated self-reported PTSD and depression symptoms and greater caregiver-rated internalizing symptoms compared to the control adolescent girls. Comparison of DERS Scores between Child Abuse and Control Groups Between-group comparisons, adjusting for age, verbal IQ, and ethnicity, demonstrated significantly higher scores among the child abuse group for the DERS total score (t(76) = 4.5, p < .001) as well as all subscale scores: nonacceptance
- 30. (t = 3.6(76), p < .001), goal-directed behavior (t = 3.8(76), p < .001), impulse control (t = 5.1(76), p < .001), strategies (t = 4.0(76), p < .001), and clarity (t = 2.2(76), p = .03). Table 1 lists means and SD of the total score and subscale scores for each group. Mediation Analyses among the Child Abuse Group A summary of mediation analyses across the dependent mea- sures is provided in Table 3. All analyses reported below con- trolled for age, verbal IQ, and ethnicity. Regarding path a (which is identical across the dependent measures), there was a significant positive relation between child abuse sever- ity and PTSD symptom severity (t(56) = 3.08, p < .003). Regarding path b across the dependent measures, there were significant relations between DERS total score and PTSD symptom severity (t = 3.94(55), p < .001), depression severity (t = 7.8(55), p < .001), and caregiver-rated internalizing symp- toms (t = 2.14(55), p = .04) upon controlling for child abuse severity. Regarding path c across the dependent measures, there were significant positive relations between child abuse severity and PTSD symptom severity (t = 6.3(56), p < .001), depression severity (t = 3.5(56), p < .001), and caregiver-rated internalizing symptoms (t = 4.3(56), p < .001). The indirect pathways ab (product of path a and b) were significantly greater than zero across the dependent measures (see Table 3), demonstrating that the indirect pathway from child abuse severity to the dependent measure through DERS total score significantly mediates the direct relation between child abuse severity and each dependent measure. However, path c’ remained significant for each dependent measures, indicating the robustness of the direct relationship between child abuse exposure and clinical symptom severity. Discussion
- 31. Overall Study The goals of this study were to examine emotion regulation as a possible mediator for the relationship between child abuse severity and PTSD/depression severity in a sample of adoles- cent females. This study aimed to address several important limitations in the current literature by examining adolescents with a high degree of abuse exposure, including a comparison group of adolescents without trauma exposure, and utilizing both self- and caregiver-report measures. Adolescents ex- posed to child abuse demonstrated greater difficulties in all aspects of emotion regulation relative to control females, as has been previously demonstrated in adult and adolescent samples. As hypothesized, emotion regulation significantly mediated the relationship between child abuse severity and symptoms of posttraumatic stress and depression. Moreover, these results do not appear to be related to reporter bias, as self-reported emotion regulation also mediated the relation- ship between child abuse severity and caregiver-reported in- ternalizing symptoms. These results strengthen previous find- ings from other populations, emphasizing the mediating role of emotion regulation in the occurrence of pathological symp- toms in adolescents who are exposed to trauma. The current results further supports prior data suggesting that emotion reg- ulation potentially operates as a transdiagnostic risk factor for mental health difficulties (McLaughlin et al. 2011) by exam- ining a heavily-traumatized population and including post- traumatic symptoms and caregiver-reported measures. Research Implications Although exposure to traumatic events is necessary in the de- velopment of PTSD and an established risk factor in the 570 J Fam Viol (2017) 32:565–575
- 32. development of depression, many individuals who experience child abuse do not go on to develop these symptoms. Though the rate of PTSD varies by type of trauma experienced, a meta- analysis conducted by Alisic et al. (2014) found that children and adolescents who appear most at risk are females who ex- perience interpersonal trauma, such as the abusive events in- cluded in the current study (Alisic et al. 2014). Specifically, they found that 32.9% of females who had been exposed to interpersonal trauma met criteria for PTSD. Given the variety of outcomes in presentation that can occur in individuals who have experienced abuse, continued work examining mediators remains an important goal for risk-factor research. Specifically, future work should examine how established mediators (e.g., emotion regulation, abuse characteristics) work in concert to confer risk for impairing maladaptive symptoms associated with experiencing abuse. For example, emotion regulation should be tested as a mediator for other types of traumatic events, such as natural disasters or motor vehicle accidents. Moreover, established mediators should be confirmed through longitudinal design, in order to establish the timing in which the Table 3 Results of mediation regression analyses across the three dependent measures Dependent measure Mediation path B t (Confidence interval) p PTSD a .55 3.08 .003 b 1.1 3.94 <.001
- 33. c 2.57 6.3 <.001 c’ 1.82 4.77 <.001 a x b indirect path .61 95% CI = .16–1.11 <.05 Depression a .55 3.08 .003 b 1.2 7.8 <.001 c 1.05 3.5 <.001 c’ .41 2.02 .048 a x b indirect path .65 95% CI = .22–1.14 <.05 Internalizing symptoms* a .55 3.08 .003 b .52 2.14 .04 c 1.38 4.3 <.001 c’ 1.08 3.2 .002 a x b indirect path .29 95% CI = .01–.65 <.05 Age, verbal IQ, and ethnicity were included as covariates in all analyses. These analyses were conducted among abuse-exposed adolescents only (n = 61) *Symptoms are caregiver-reported
- 34. Child Abuse Severity Fig. 1 Illustration of the generic mediation framework and the hypothesized mediation pathway in the current study J Fam Viol (2017) 32:565–575 571 development of mental health symptoms, mediators (e.g., emo- tion regulation abilities), and abusive incidents occur. Clinical Implications Early and middle adolescence represent time periods of devel- opment in emotion regulation capacities as well as mental health disorders, and thus, are sensitive times in which inter- ventions may produce long-lasting change. Given the potential problematic trajectory of individuals who have been exposed to child abuse, intervention to alter this course is crucial. There is a current call in the literature to examine mediators for treat- ment responsiveness in high-risk populations. Particularly with PTSD, research on adult individuals with severe symptoms (mirroring our population in a different developmental period) demonstrates that roughly 40% - 50% of individuals with chronic PTSD symptoms fail to meet criteria for functional improvement or symptom discontinuation after receiving a course of treatment (Foa et al. 2002). Given that emotion reg- ulation difficulties may mediate symptom presentation, per- haps they also may mediate treatment responsiveness. Addressing emotion dysregulation could be an important pre- ventative area, as it associated with a variety of mental health
- 35. disorders. Moreover, given the high comorbidity rate between PTSD and other mental health conditions, traumatized youth could represent an ideal sample to target for such interventions. However, there is disagreement in the field as to whether the current evidence-based interventions for adolescent trau- ma (e.g., Trauma-Focused Cognitive Behavioral Therapy, TF- CBT) adequately build emotion regulation or whether a phase-based approach including treatments specifically targeting poor emotion regulation should be used. Indeed, studies with adult PTSD patients have found greater improve- ment in PTSD symptoms by adding a component specifically addressing emotion regulation to the typical course of trauma treatment (Bryant et al. 2013; Cloitre et al. 2010). For cases of complex trauma, the creators of TF-CBT have suggested ex- tending the emotion regulation/stabilization phase of treat- ment, acknowledging the deficits in these skills for highly traumatized youth (Cohen et al. 2012). However, limited re- search has been done on the traditional and extended treatment models of TF-CBT related to efficacy in building emotion regulation. This is an important empirical question that should be examined in future work. Indeed, emotion regulation could be an important area to target within family work for a variety of reasons. First, genetic studies on emotion regulation (specifically alexithymia) sug- gest that between 30% and 40% of the variability within this trait can be accounted for by genetic influences (Jørgensen et al. 2007; Picardi et al. 2011), suggesting that parents/caregivers of these children may also struggle with regulating emotions. Second, developmental theorists posit that emotion regulation during infancy and childhood is largely influenced by parental behaviors (see Shipman et al. 2007 for a review), suggesting a model in which parenting behaviors confer risk for poor emo- tion regulation, subsequently conferring risk for developing
- 36. emotional or behavioral symptoms. Taken together, these findings suggest that targeting emotion regulation and its’ impact on parenting may help caregivers to support adolescent gains within treatment and improve the caregiver-child relation- ship. Although our study was not able to explicitly test the development of emotion regulation skills or symptoms over time, as it was cross-sectional in nature, it underscores the im- portant role these skills have in impacting the association be- tween prior adverse life events and current pathological symp- tom presentations. Future research should examine whether parent/caregiver emotion regulation mediates the relationship between childhood abuse and child maladaptive symptoms and whether these symptoms improve during evidence-based youth trauma treatment. Fortunately, most evidence-based trauma treatments for youth (e.g. Trauma-Focused Cognitive Behavioral Therapy, Child Parent Psychotherapy) explicitly in- volve considerable parent/caregiver work and thus already pro- vide the framework to target parent/caregiver emotion regula- tion, if needed. Study Strengths The greatest strength of this study is our unique sample, as we examined adolescent females with a high degree of child abuse severity. Prior to this study, emotion regulation as a mediating factor in the relationship between child abuse and PTSD/depressive symptoms had not been established in highly-impaired adolescent samples, which are more repre- sentative of those that present to treatment. Prevalence rates reported by a variety of mental health clinics within the National Traumatic Stress Network suggest an average of 3– 4 trauma types experienced by children ages 1.5 to 18 years (Greeson et al. 2014). By comparison, adolescent girls in the current sample were exposed to 5.3 child abusive traumas on average; therefore, our sample is high-risk and largely repre- sentative of highly-impaired individuals who present for treat-
- 37. ment. Moreover, this sample was diverse in nature, allowing for generalization of these findings to a broader patient popu- lation. We also controlled for several confounding variables, including verbal IQ, age, and ethnicity, and can therefore be more confident of the relationship between these variables. Finally, utilizing caregiver- and self-report measures of mental health symptoms helps to avoid reporter bias, as one could easily argue that individuals with poor emotion regulation may be biased in their self-report of emotional symptoms. Study Limitations Study strengths should be considered along with limitations. Due to the cross-sectional nature of the study, true mediation 572 J Fam Viol (2017) 32:565–575 was not able to be measured. This would require a longitudi- nal study that could fully establish the timing of abuse events and symptom development. Despite this limitation, the results are similar to previous findings on adult and undergraduate samples without the cost and time of conducting a longitudi- nal study with a difficult population to track and measure. Examining highly-impaired individuals often leads to a small- er sample size, as is this case with our study. However, statis- tical measures were taken to correct for the smaller sample, including bootstrapping techniques and iterative least squares regression to minimize the impact of outliers. Moreover, al- though the sample was small, recruitment took place within the community in addition to trauma-specific clinics and the participants were ethnically-diverse and largely representative of the geographical location of the current study. Our study also included several covariates (e.g., age, verbal IQ, ethnici- ty), but did not include other variables that may impact this
- 38. relationship (such as income level, household composition) that would be important to include in future studies. Therefore, these results should be replicated in a larger sam- ple, in order to ensure the generalizability of our findings. Moreover, our study focused on early and middle adolescence as important developmental periods for both emotion regula- tion abilities and mental health disorders. It would be impor- tant to assess whether these findings would remain true for other periods of adolescence. Also, this study made use of subjective measures of all variables, which are inherently sus- ceptible to individual bias. Future work should examine this relationship using objective measures of emotion regulation. Similarly, no caregiver-report measure of emotion regulation was obtained, which could have offered a more comprehen- sive examination of these deficits. It is also important to note that our measure of child abuse severity was defined as the number of categories of child abuse to which the child was exposed, as opposed to the total number of times that the child has been abused independent of the number of categories. Our methodology also focused on the number of categories so that the child would only have to provide ‘yes/no’ responses to whether a given category occurred, towards the goal of in- creasing reliability, given that these were retrospective reports of child abuse exposure. Assessing categories of trauma, as opposed to number of traumatic episodes experienced is also consistent with prior research (Kolassa et al. 2010a, b). However, it is certainly possible that a child who was only exposed to one category of child abuse could be exposed multiple times to that category (e.g., several episodes of witnessing domestic violence within this category). As such, future research is needed that spans a range of methodology for measuring trauma exposure to establish the robustness of the current findings. Finally, our choice to frame abuse expo- sure questions in a Byes/no^ format without asking partici- pants to elaborate further also prevented the inclusion of sev- eral other factors that would be important to examine in future
- 39. studies, including age of exposure, relationship to perpetrator, or perception of betrayal associated with the abuse. Experiences of child abuse put youth at great risk for a multitude of mental and physical health concerns. Work that examines mediators in symptom presentations for highly- traumatized populations can directly inform care for those who arguably need it most. Our findings underscore the im- portance of examining individual traits, such as emotion reg- ulation, as potential mediators for the relationship between a history of child abuse exposure and current symptoms of post- traumatic stress and depression. These results also support emotion regulation skills training as an important point of intervention for youth with extensive child abuse exposure. Acknowledgements This research was supported in part by grants MH097784 and DA036360 from the National Institutes of Health. References Achenbach, T. M. (1991). Integrative guide to the 1991 CBCL/4–18, YSR, and TRF profiles. Burlington: University of Vermont, Department of Psychology. Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion- regulation strategies across psychopathology: A meta-analytic re- view. Clinical Psychology Review, 30, 217–237. doi:10.1016/j. cpr.2009.11.004.
- 40. Alisic, E., Zalta, A. K., van Wesel, F., Larsen, S. E., Hafstad, G. S., Hassanpour, K., & Smid, G. E. (2014). Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: Meta- analysis. The British Journal of Psychiatry, 204(5), 335–340. doi:10.1192 /bjp.bp.113.131227. American Academy of Pediatrics (2015). Stages of Adolescence. Retrieved from https://www.healthychildren.org/English/ages- stages/teen/Pages/Stages-of-Adolescence.aspx. Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., & O’Farrill-Swails, L. (2005). Single versus multi-type maltreatment: An examination of the long-term effects of child abuse. Journal of Aggression, Maltreatment & Trauma, 11, 29–52. doi:10.1300/J146v11n04_02. Bardeen, J. R., Fergus, T. A., & Orcutt, H. K. (2012). An examination of the latent structure of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 34(3), 382–392. doi:10.1007/s10862-012-9280-y. Baron, R. M., & Kenny, D. A. (1986). The moderator mediator variable distinction in social psychological-research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. doi:10.1037//0022- 3514.51.6.1173.
- 41. Blakemore, S. (2008). The social brain in adolescence. Nature Reviews Neuroscience, 9, 267–277. doi:10.1038/nrn2353. Blakemore, S., & Choudhury, S. (2006). Development of the adolescent brain: Implications for executive function and social cognition. Journal of Child Psychology and Psychiatry, 47, 296–312. doi:10.1111/j.1469-7610.2006.01611.x. Blumenthal, H., Blanchard, L., Feldner, M. T., Babson, K. A., Leen- Feldner, E. W., & Dixon, L. (2008). Traumatic event exposure, posttraumatic stress, and substance use among youth: A critical re- view of the empirical literature. Current Psychiatry Reviews, 4, 228– 254. doi:10.2174/157340008786576562. Briere, J., & Jordan, C. E. (2009). Childhood maltreatment, intervening variables, and adult psychological difficulties in women: An J Fam Viol (2017) 32:565–575 573 http://dx.doi.org/10.1016/j.cpr.2009.11.004 http://dx.doi.org/10.1016/j.cpr.2009.11.004 http://dx.doi.org/10.1192/bjp.bp.113.131227 http://dx.doi.org/10.1192/bjp.bp.113.131227 https://www.healthychildren.org/English/ages- stages/teen/Pages/Stages-of-Adolescence.aspx https://www.healthychildren.org/English/ages- stages/teen/Pages/Stages-of-Adolescence.aspx http://dx.doi.org/10.1300/J146v11n04_02 http://dx.doi.org/10.1007/s10862-012-9280-y http://dx.doi.org/10.1037//0022-3514.51.6.1173
- 42. http://dx.doi.org/10.1038/nrn2353 http://dx.doi.org/10.1111/j.1469-7610.2006.01611.x http://dx.doi.org/10.2174/157340008786576562 overview. Trauma, Violence & Abuse, 10, 375–388. doi:10.1177 /1524838009339757. Bryant, R. A., Mastrodomenico, J. J., Hopwood, S. S., Kenny, L. L., Cahill, C. C., Kandris, E. E., & Taylor, K. K. (2013). Augmenting cognitive behaviour therapy for post-traumatic stress disorder with emotion tolerance training: A randomized controlled trial. Psychological Medicine, 43(10), 2153–2160. doi:10.1017 /S0033291713000068. Choi, J., & Oh, K. (2014). Cumulative childhood trauma and psycholog- ical maladjustment of sexually abused children in Korea: Mediating effects of emotion regulation. Child Abuse and Neglect, 38(2), 296– 303. doi:10.1016/j.chiabu.2013.09.009. Cisler, J. M., Amstadter, A. B., Begle, A. M., Resnick, H. S., Danielson, C. K., & Saunders, B. E. (2011a). A prospective examination of the relationships between PTSD, exposure to assaultive violence, and cigarette smoking among a national sample of adolescents. Addictive Behaviors, 36(10), 994–1000. doi:10.1016/j. addbeh.2011.05.014.
- 43. Cisler, J. M., Amstadter, A. B., Begle, A. M., Resnick, H. S., Danielson, C. K., & Saunders, B. E. (2011b). PTSD symptoms, potentially traumatic event exposure, and binge drinking: A prospective study with a national sample of adolescents. Journal of Anxiety Disorders, 25(7), 978–987. doi:10.1016/j.janxdis.2011.06.006. Cisler, J. M., Begle, A. M., Amstadter, A. B., Resnick, H. S., Danielson, C. K., & Saunders, B. E. (2012). Exposure to interpersonal violence and risk for PTSD, depression, delinquency, and binge drinking among adolescents: Data from the NSA-R. Journal of Traumatic Stress, 25(1), 33–40. doi:10.1002/jts.21672. Cisler, J. M., Sigel, B. A., Steele, J. S., Smitherman, S., Vanderzee, K., Pemberton, J., Kramer, T.L., & Kilts, C. D. (2016). Changes in functional connectivity of the amygdala during cognitive reappraisal predict symptom reduction during trauma-focused cognitive– behav- ioral therapy among adolescent girls with post-traumatic stress dis- order. Psychological Medicine, 46(14), 3013–3023. doi:10.1017 /S0033291716001847. Cloitre, M., Stovall-McClough, K., Nooner, K., Zorbas, P., Cherry, S., Jackson, C. L., Gan, W., & Petkova, E. (2010). Treatment for PTSD related to childhood abuse: A randomized controlled trial. The American Journal of Psychiatry, 167(8), 915–924. doi:10.1176 /appi.ajp.2010.09081247.
- 44. Cohen, J. A., Mannarino, A. P., Kliethermes, M., & Murray, L. A. (2012). Trauma-focused CBT for youth with complex trauma. Child Abuse & Neglect, 36(6), 528–541. doi:10.1016/j.chiabu.2012.03.007. Crow, T., Cross, D., Powers, A., & Bradley, B. (2014). Emotion dysreg- ulation as a mediator between childhood emotional abuse and cur- rent depression in a low-income African-American sample. Child Abuse & Neglect. doi:10.1016/j.chiabu.2014.05.015. Donnelly, C., & Amaya-Jackson, L. (2004). Pediatric post- traumatic stress disorder. In J. Weiner & M. Dulcan (Eds.), The American Psychiatric Publishing textbook of child and adolescent Psychiatry (3rd ed.). Washington, DC: American Psychiatric Publishing. Ehring, T., & Quack, D. (2010). Emotion regulation difficulties in trauma survivors: The role of trauma type and ptsd symptom severity. Behavior Therapy, 41(4), 587–598. doi:10.1016/j.beth.2010.04.004. Fairholme, C. P., Nosen, E. L., Nillni, Y. I., Schumacher, J. A., Tull, M. T., & Coffey, S. F. (2013). Sleep disturbance and emotion dysregulation as transdiagnostic processes in a comorbid sample. Behaviour Research and Therapy, 51(9), 540–546. doi:10.1016/j.brat.2013.05.014.
- 45. Foa, E., Zoellner, L. A., Feeny, N. C., Hembree, E. A., & Alvarez- Conrad, J. (2002). Does imaginal exposure exacerbate PTSD symp- toms? Journal of Consulting and Clinical, 70, 1022–1028. doi:10.1037//0022-006X.70.4.1022. Goldsmith, R. E., Chesney, S. A., Heath, N. M., & Barlow, M. (2013). Emotion regulation difficulties mediate associations between betray- al trauma and symptoms of posttraumatic stress, depression, and anxiety. Journal of Traumatic Stress, 26(3), 376–384. doi:10.1002 /jts.21819. Gratz, K. L., Bornovalova, M. A., Delany-Brumsey, A., Nick, B., & Lejuez, C. W. (2007). A laboratory-based study of the relationship between childhood abuse and experiential avoidance among inner- city substance users: The role of emotional nonacceptance. Behavior Therapy, 38(3), 256–268. doi:10.1016/j.beth.2006.08.006. Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emo- tion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26, 41– 55. doi:10.1023/B:JOBA.0000007455.08539.94.
- 46. Greeson, J., Briggs, E., Layne, C., Belcher, H., Ostrowski, S., Kim, S., Lee, R., Vivrette, R., Pynoos, R., & Fairbank, J. (2014). Traumatic childhood experiences in the 21st century: Broadening and building on the ACE studies with data from the National Child Traumatic Stress Network. Journal of Interpersonal Violence, 29(3), 536– 556. doi:10.1177/0886260513505217. Greif Green, J., McLaughlin, K. A., Berglund, P. A., Gruber, M. J., Sampson, N. A., Zaslavsky, A. M., & Kessler, R. C. (2010). Childhood adversities and adult psychiatric disorders in the National Comorbidity Survey Replication. I: Associations with first onset of DSM–IV disorders. Archives of General Psychiatry, 67, 113–123. doi:10.1001/archgenpsychiatry.2009.186. Herts, K. L., McLaughlin, K. A., & Hatzenbuehler, M. L. (2012). Emotion dysregulation as a mechanism linking stress exposure to adolescent aggressive behavior. Journal of Abnormal Child Psychology, 40(7), 1111–1122. doi:10.1007/s10802-012-9629-4. Jørgensen, M., Zachariae, R., Skytthe, A., & Kyvik, K. (2007). Genetic and environmental factors in alexithymia: A population-based study of 8,785 Danish twin pairs. Psychotherapy and Psychosomatics, 76(6), 369–375. doi:10.1159/000107565. Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., &
- 47. Moreci, P. (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child and Adolescent Psychiatry, 36(7), 980–988. doi:10.1097/00004583-199707000-00021. Kilpatrick, D. G., Acierno, R., Saunders, B., Resnick, H. S., Best, C. L., & Schnurr, P. P. (2000). Risk factors for adolescent substance abuse and dependence: Data from a national sample. Journal of Consulting and Clinical Psychology, 68(1), 19–30. doi:10.1037 //0022-006X.68.1.19. Kilpatrick, D. G., Ruggiero, K. J., Acierno, R., Saunders, B. E., Resnick, H. S., & Best, C. L. (2003). Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: Results from the National Survey of adolescents. Journal of Consulting and Clinical Psychology, 71(4), 692–700. doi:10.1037/0022-006 X.71.4.692. Kim, J., & Cicchetti, D. (2010). Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathol- ogy. Journal of Child Psychology and Psychiatry, 51, 706–716. doi:10.1111/j.1469-7610.2009.02202.x. Kolassa, I. T., Ertl, V., Eckart, C., Glockner, F., Kolassa, S., & Papassotiropoulos, A. (2010a). Association study of trauma load and SLC6A4 promoter polymorphism in posttraumatic stress disor-
- 48. der: Evidence from survivors of the Rwandan genocide. Journal of Clinical Psychiatry, 71(5), 543–547. doi:10.4088/JCP.08m04787blu. Kolassa, I. T., Kolassa, S., Ertl, V., Papassotiropoulos, A., & De Quervain, D. J. (2010b). The risk of posttraumatic stress disorder after trauma depends on traumatic load and the catechol-o- methyltransferase Val(158)met polymorphism. Biological Psychiatry, 67(4), 304–308. doi:10.1016/j.biopsych.2009.10.009. Kring, A. M., & Werner, K. H. (2004). Emotion regulation and psycho- pathology. In P. Philippot & R. S. Feldman (Eds.), The regulation of 574 J Fam Viol (2017) 32:565–575 http://dx.doi.org/10.1177/1524838009339757 http://dx.doi.org/10.1177/1524838009339757 http://dx.doi.org/10.1017/S0033291713000068 http://dx.doi.org/10.1017/S0033291713000068 http://dx.doi.org/10.1016/j.chiabu.2013.09.009 http://dx.doi.org/10.1016/j.addbeh.2011.05.014 http://dx.doi.org/10.1016/j.addbeh.2011.05.014 http://dx.doi.org/10.1016/j.janxdis.2011.06.006 http://dx.doi.org/10.1002/jts.21672 http://dx.doi.org/10.1017/S0033291716001847 http://dx.doi.org/10.1017/S0033291716001847 http://dx.doi.org/10.1176/appi.ajp.2010.09081247 http://dx.doi.org/10.1176/appi.ajp.2010.09081247 http://dx.doi.org/10.1016/j.chiabu.2012.03.007 http://dx.doi.org/10.1016/j.chiabu.2014.05.015
- 49. http://dx.doi.org/10.1016/j.beth.2010.04.004 http://dx.doi.org/10.1016/j.brat.2013.05.014 http://dx.doi.org/10.1037//0022-006X.70.4.1022 http://dx.doi.org/10.1002/jts.21819 http://dx.doi.org/10.1002/jts.21819 http://dx.doi.org/10.1016/j.beth.2006.08.006 http://dx.doi.org/10.1023/B:JOBA.0000007455.08539.94 http://dx.doi.org/10.1177/0886260513505217 http://dx.doi.org/10.1001/archgenpsychiatry.2009.186 http://dx.doi.org/10.1007/s10802-012-9629-4 http://dx.doi.org/10.1159/000107565 http://dx.doi.org/10.1097/00004583-199707000-00021 http://dx.doi.org/10.1037//0022-006X.68.1.19 http://dx.doi.org/10.1037//0022-006X.68.1.19 http://dx.doi.org/10.1037/0022-006X.71.4.692 http://dx.doi.org/10.1037/0022-006X.71.4.692 http://dx.doi.org/10.1111/j.1469-7610.2009.02202.x http://dx.doi.org/10.4088/JCP.08m04787blu http://dx.doi.org/10.1016/j.biopsych.2009.10.009 emotion (pp. 359–385). Mahwah, New Jersey: Lawrence Erlbaum Associates Publishers. Larson, R., & Richards, M. H. (1991). Daily companionship in late child- hood and early adolescence: Changing developmental contexts. Child Development, 62, 284–300. doi:10.2307/1131003. Lenow, J. K., Steele, J. S., Smitherman, S., Kilts, C. D., & Cisler, J. M. (2014). Attenuated behavioral and brain responses to trust violations among child abused adolescent girls. Psychiatry Research: Neuroimaging, 223, 1–8.
- 50. doi:10.1016/j.pscychresns.2014.04.005. Lilly, M. M., & Lim, B. (2013). Shared pathogeneses of posttrauma pa- thologies: Attachment, emotion regulation, and cognitions. Journal of Clinical Psychology, 69(7), 737–748. doi:10.1002/jclp.21934. MacKinnon, D. P., Fairchild, A. J., & Fritz, M. S. (2007). Mediation analysis. Annual Review of Psychology, 58, 593–614. doi:10.1146 /annurev.psych.58.110405.085542. McLaughlin, K. A., Hatzenbuehler, M. L., Mennin, D. S., & Nolen- Hoeksema, S. (2011). Emotion dysregulation and adolescent psy- chopathology: A prospective study. Behaviour Research and Therapy, 49(9), 544–554. doi:10.1016/j.brat.2011.06.003. Patton, G., Coffey, C., Romaniuk, H., Mackinnon, A., Carlin, J., Degenhardt, L., Olsson, C., & Moran, P. (2014). The prognosis of common mental disorders in adolescents: A 14-year prospective cohort study. The Lancet, 383, 1404–1411. doi:10.1016/S0140- 6736(13)62116-9. Paus, T., Keshavan, M., & Giedd, J. N. (2008). Why do many psychiatric disorders emerge during adolescence? Nature Reviews Neuroscience, 9, 947–957. doi:10.1038/nrn2513. Picardi, A., Fagnani, C., Gigantesco, A., Toccaceli, V., Lega, I., & Stazi, M. (2011). Genetic influences on alexithymia and their
- 51. relationship with depressive symptoms. Journal of Psychosomatic Research, 71(4), 256–263. doi:10.1016/j.jpsychores.2011.02.016. Pollak, S. D., & Sinha, P. (2002). Effects of early experience on children's recognition of facial displays of emotion. Developmental Psychology, 38(5), 784–791. doi:10.1037/0012-1649.38.5.784. Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strat- egies for assessing and comparing indirect effects in multiple medi- ator models. Behavior Research Methods, 40(3), 879–891. doi:10.3758/BRM.40.3.879. Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Janavs, J., Bannon, Y., & Rogers, J. E. (2010). Reliability and validity of the Mini internation- al neuropsychiatric interview for children and adolescents (MINI- KID). Journal of Clinical Psychiatry, 71(3), 313–326. doi:10.4088 /JCP.09m05305whi. Shipman, K. L., Schneider, R., Fitzgerald, M. M., Sims, C., Swisher, L., & Edwards, A. (2007). Maternal emotion socialization in maltreating and non-maltreating families: Implications for children's emotion regulation. Social Development, 16(2), 268–285. doi:10.1111/j.1467-9507.2007.00384.x. Shipman, K., Zeman, J., Penza, S., & Champion, K. (2000). Emotion
- 52. management skills in sexually maltreated and nonmaltreated girls: A developmental psychopathology perspective. Development and Psychopathology, 12(1), 47–62. doi:10.1017/S0954579400001036. Spinrad, T., Eisenberg, N., Cumberland, A., Fabes, R., Valiente, C., Shepard, S., Reiser, M., Losoya, S., & Guthrie, I. (2006). Relation of emotion-related regulation to children's social competence: A longitu- dinal study. Emotion, 6, 498–510. doi:10.1037/1528- 3542.6.3.498. Steinberg, L., & Avenevoli, S. (2000). The role of context in the devel- opment of psychopathology: A conceptual framework and some speculative propositions. Child Development, 71, 66–74. doi:10.1111/1467-8624.00119. Steinberg, A. M., Brymer, M. J., Decker, K. B., & Pynoos, R. S. (2004). The University of California at Los Angeles post-traumatic stress disorder Reaction Index. Current Psychiatry Reports, 6(2), 96– 100. doi:10.1007/s11920-004-0048-2. Steinberg, A. M., Brymer, M. J., Kim, S., Briggs, E. C., Ippen, C. G., & Ostrowski, S. A. (2013). Psychometric properties of the UCLA PTSD Reaction Index: Part I. Journal of Traumatic Stress, 26(1), 1–9. doi:10.1002/Jts.21780.
- 53. Sundermann, J. M., & DePrince, A. P. (2015). Maltreatment characteris- tics and emotion regulation (ER) difficulties as predictors of mental health symptoms: Results from a community-recruited sample of female adolescents. Journal of Family Violence, 30(3), 329– 338. doi:10.1007/s10896-014-9656-8. Tull, M. T., Barrett, H. M., McMillan, E. S., & Roemer, L. (2007). A preliminary investigation of the relationship between emotion regu- lation difficulties and posttraumatic stress symptoms. Behavior Therapy, 38, 303–313. doi:10.1016/j.beth.2006.10.001. U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2015). Child Maltreatment 2013. Available from http://www.acf.hhs.gov/programs/cb/research- data- technology/statistics-research/child-maltreatment. Ullman, S. E., Peter-Hagene, L. C., & Relyea, M. (2014). Coping, emo- tion regulation, and self-blame as mediators of sexual abuse and psychological symptoms in adult sexual assault. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations For Victims, Survivors, & Offenders, 23(1), 74–93. doi:10.1080 /10538712.2014.864747. Weinberg, A., & Klonsky, E. D. (2009). Measurement of
- 54. emotion dys- regulation in adolescents. Psychological Assessment, 21(4), 616– 621. doi:10.1037/a0016669. Weiss, N. H., Tull, M. T., Viana, A. G., Anestis, M. D., & Gratz, K. L. (2012). Impulsive behaviors as an emotion regulation strategy: Examining associations between PTSD, emotion dysregulation, and impulsive behaviors among substance dependent inpatients. Journal of Anxiety Disorders, 26(3), 453–458. doi:10.1016/j. janxdis.2012.01.007. J Fam Viol (2017) 32:565–575 575 http://dx.doi.org/10.2307/1131003 http://dx.doi.org/10.1016/j.pscychresns.2014.04.005 http://dx.doi.org/10.1002/jclp.21934 http://dx.doi.org/10.1146/annurev.psych.58.110405.085542 http://dx.doi.org/10.1146/annurev.psych.58.110405.085542 http://dx.doi.org/10.1016/j.brat.2011.06.003 http://dx.doi.org/10.1016/S0140-6736(13)62116-9 http://dx.doi.org/10.1016/S0140-6736(13)62116-9 http://dx.doi.org/10.1038/nrn2513 http://dx.doi.org/10.1016/j.jpsychores.2011.02.016 http://dx.doi.org/10.1037/0012-1649.38.5.784 http://dx.doi.org/10.3758/BRM.40.3.879 http://dx.doi.org/10.4088/JCP.09m05305whi http://dx.doi.org/10.4088/JCP.09m05305whi http://dx.doi.org/10.1111/j.1467-9507.2007.00384.x http://dx.doi.org/10.1017/S0954579400001036 http://dx.doi.org/10.1037/1528-3542.6.3.498 http://dx.doi.org/10.1111/1467-8624.00119 http://dx.doi.org/10.1007/s11920-004-0048-2 http://dx.doi.org/10.1002/Jts.21780 http://dx.doi.org/10.1007/s10896-014-9656-8
- 55. http://dx.doi.org/10.1016/j.beth.2006.10.001 http://www.acf.hhs.gov/programs/cb/research-data- technology/statistics-research/child-maltreatment http://www.acf.hhs.gov/programs/cb/research-data- technology/statistics-research/child-maltreatment http://dx.doi.org/10.1080/10538712.2014.864747 http://dx.doi.org/10.1080/10538712.2014.864747 http://dx.doi.org/10.1037/a0016669 http://dx.doi.org/10.1016/j.janxdis.2012.01.007 http://dx.doi.org/10.1016/j.janxdis.2012.01.007 Journal of Family Violence is a copyright of Springer, 2017. All Rights Reserved. Emotion...AbstractIntroductionChild AbuseChild Abuse and Associated DifficultiesEmotion RegulationThe Relationship between Emotion Regulation and Child AbuseThe Current StudyMethodParticipantsAssessmentsStatistical AnalysesResultsParticipant Characteristics and Preliminary AnalysesComparison of DERS Scores between Child Abuse and Control GroupsMediation Analyses among the Child Abuse GroupDiscussionOverall StudyResearch ImplicationsClinical ImplicationsStudy StrengthsStudy LimitationsReferences Evaluating a Research Article/Research Article Summary The articles reviewed for this assignment must report the results of someone's research in an area of social research. The research should have been carried out by the author(s). The article must be directed at a scholarly audience. Your review must be on an article reporting structured research, that is, one with variables, statistical analyses, relationships among variables, etc. The article may be about any Human Growth and Development topic you choose. Check with me if you have any doubts about your topic. The following types of articles may NOT be used: · Purely theoretical papers which discuss concepts and
- 56. propositions, but report no empirical research; · Statistical or methodological papers where data may be analyzed but the bulk of the work is on the refinement of some new measurement, statistical or modeling technique; · Review articles, which summarize the research of many different past researchers, but report no original research by the author; · Popularizations or abridged reports, commonly found in popular newsstand magazines such as Psychology Today or books of readings designed for use by undergraduates; · Extremely short reports with less than four pages devoted to methods and findings. Most research reports beginwith sections on theory and reviews of others' research, so skim the whole article or read the abstract, if there is one, to determine whether the author reports actual research he or she has done. Psychology, as is true of all scientific fields, is becoming increasingly complex in its statistical analyses. A working rule is: if you can't understand the statistical analyses presented in the results section, don't choose the article. All articles must receive my OK. No two students may review the same article. It is OK to use articles you have to read for another class, if they meet all of the above criteria. Student Name Date PSY203-82 Research Article Summary Outline for the Research Article Review When writing the research article summary use the following
- 57. outline to present the information. The sections should be labeled with the Roman numeral; however, the information should be written in complete sentences in a logical paragraph structure. The paper should be identified in the manner seen above. I. Give the Citation for the article. a. Provide the citation for the article in APA or MLA format. II. Evaluating the Introduction a. What is the chosen topic for the research paper? b. What is the purpose of the research study/paper? c. What is the hypothesis of the research study provided in the paper? III. Experimental design/Data collection a. What is the source of the data/How was the data acquired? (That is, questionnaire, intensive interview, documents, existing statistical information, observations, laboratory manipulations, field manipulations, etc.) b. Is the study a quantitative or qualitative study? c. What was the sample population? d. How was the data analyzed? (Discuss the statistical test(s) performed and what data was presented.) IV. Discussion of results a. Briefly summarize the findings and conclusions concerning the data mentioned by the author(s). V. Overall Evaluation a. Give your overall evaluation of the methods used in this article: What things were done well? What were done poorly? How much trust do you put in the findings? b. Look at this article's "packaging," that is, the theoretical introduction and the discussion or interpretation at the end. Do you feel that the actual methods and results support the theoretical and interpretive claims of the author? Why?
- 58. c. What possible ethical issues might have arisen in the process of doing this research? Do you think the researcher's ethical decisions were all justified, or are some questionable? Why? d. To sum up, what do you feel you have learned worth knowing from this article? (If your answer is "nothing", explain why.) (Please note: this question is about the article and refers to the quality of information it contains.) Research Article Summary Rubric Criteria Grading Points Score I. Research article selection (20pts.) · Article was approved by instructor. · Student included the citation for the article provided adhering to APA format. II. Content of the summary (100pts.) Student evaluated the article and presented the answers to the following questions: · What is the chosen topic for the research paper? · What is the purpose of the research study/paper? · What is the hypothesis of the research study provided in the paper? · What is the source of the data/How was the data acquired? (That is, questionnaire, intensive interview, documents, existing statistical information, observations, laboratory manipulations, field manipulations, etc.) · Is the study a quantitative or qualitative study? · What was the sample population? · How was the data analyzed? (Discuss the statistical test(s) performed and what data was presented.) · Briefly summarize the findings and conclusions concerning the data mentioned by the author(s).
- 59. III. Overall Evaluation (40 pts.) Student provided the overall evaluation of the article to include the following: · Give your overall evaluation of the methods used in this article: What things were done well? What were done poorly? How much trust do you put in the findings? · Look at this article's "packaging," that is, the theoretical introduction and the discussion or interpretation at the end. Do you feel that the actual methods and results support the theoretical and interpretive claims of the author? Why? · What possible ethical issues might have arisen in the process of doing this research? Do you think the researcher's ethical decisions were all justified, or are some questionable? Why? · To sum up, what do you feel you've learned worth knowing from this article? (If your answer is "nothing", explain why.) (Please note: this question is about the article and refers to the quality of information it contains.) IV. Content, clarity, and organization of ideas. (40pts.) Student correctly adheres to the following when submitting the final draft for grading: · Submission appropriately labeled. · No inclusion of first or second person reference (ie, no I, We, You, etc). · No more than 2 grammar mistakes. (-2pts each) · No spelling mistakes. (-2pts each) · Typed, Double spaced, Times New Roman or Arial, 10-12-pt font. Total Grade: Instructor Comments: