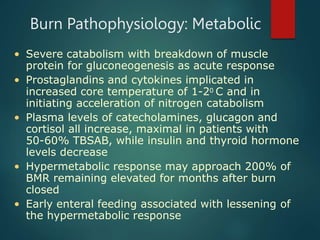
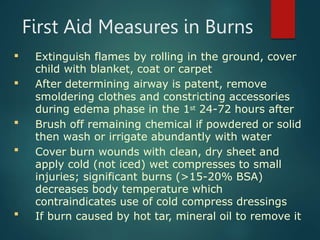
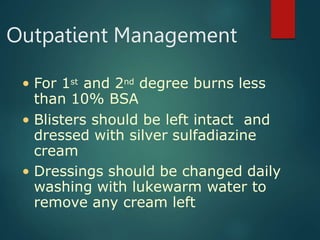
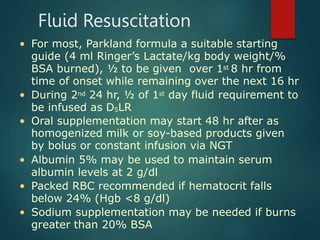
Burns are classified based on depth and extent of tissue damage. First degree burns involve only the epidermis, while second degree burns extend deeper into the dermis and may cause blistering. Third degree burns extend through the entire thickness of skin. Proper first aid and fluid resuscitation are important to prevent further tissue damage. Hospitalization is recommended for burns covering over 10% of total body surface area or involving sensitive areas like the hands, face or genitals. Management involves wound care, pain control, nutrition and physical therapy.












































![nursing management of burn wounds.. [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burns-classnotes-250310073133-5480c852-thumbnail.jpg?width=640&height=640&fit=bounds)












































