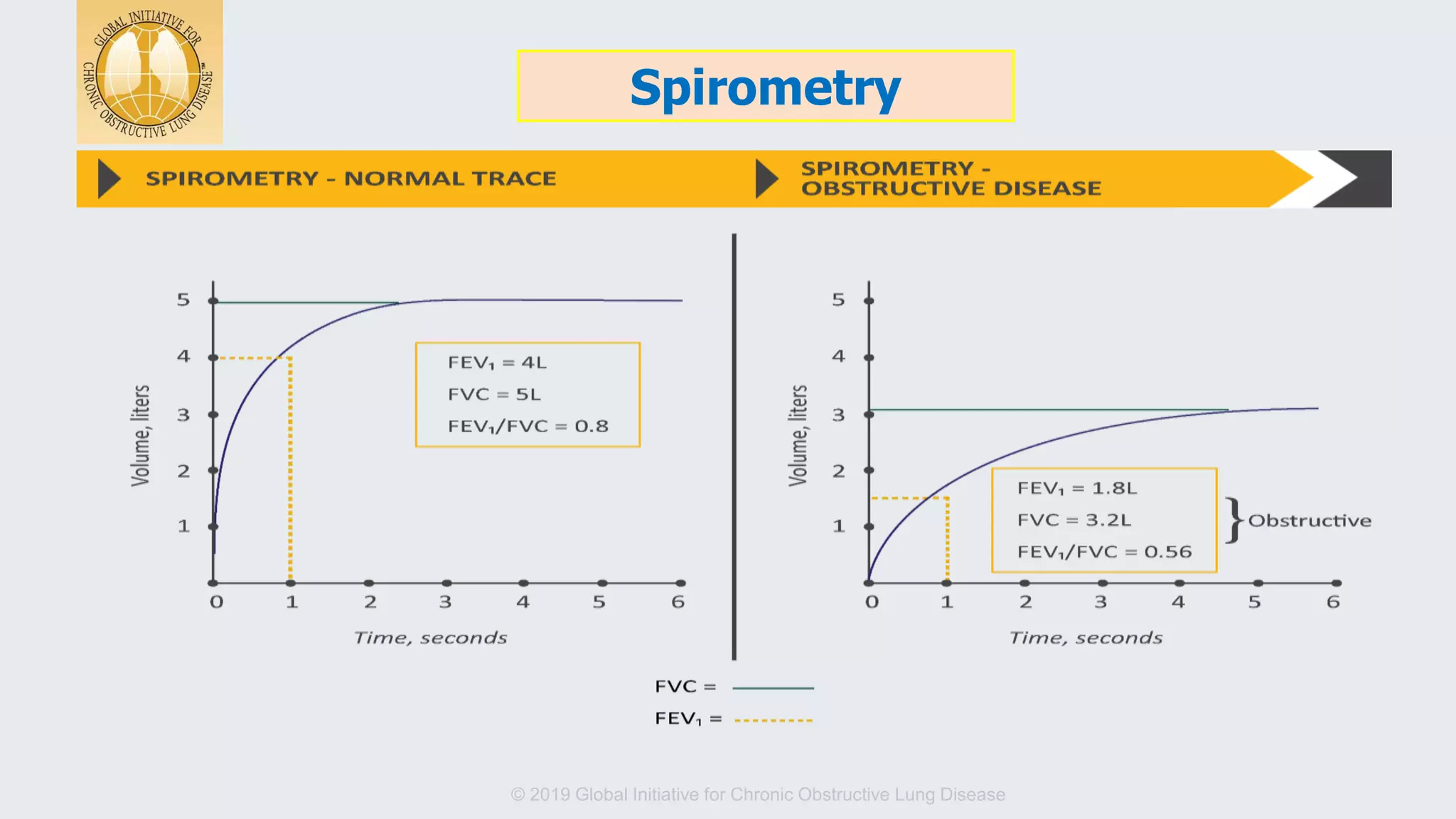
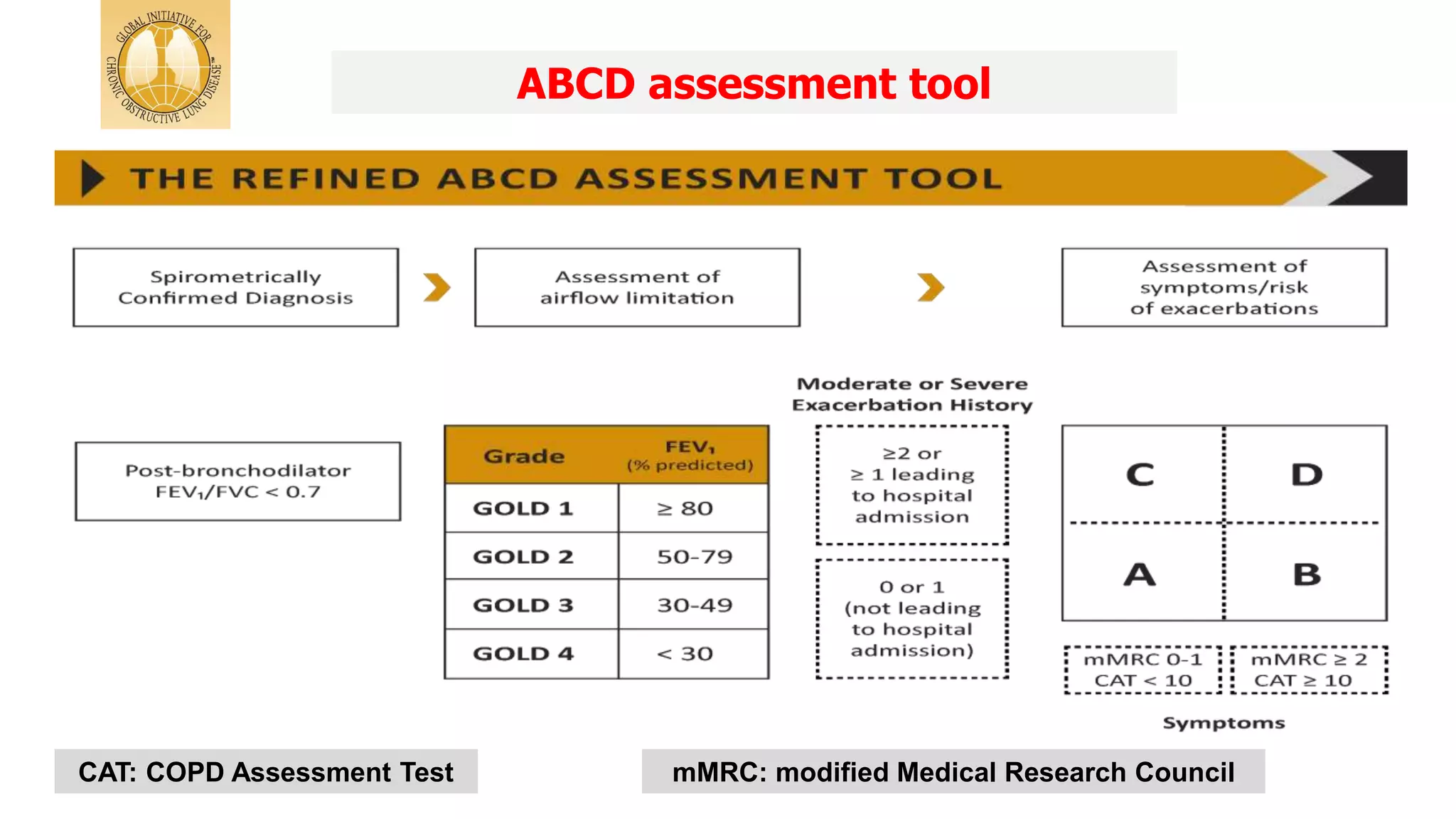
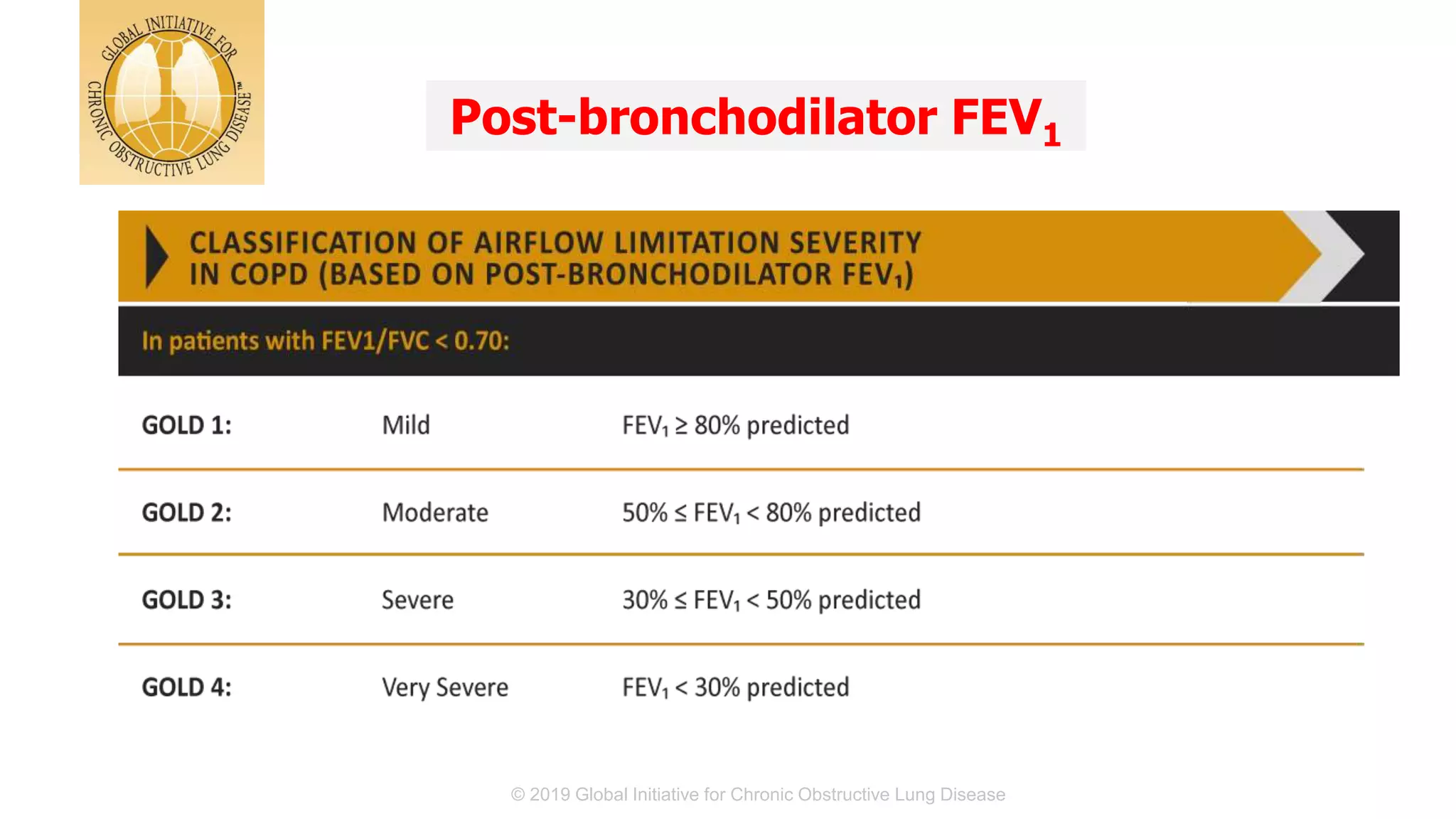
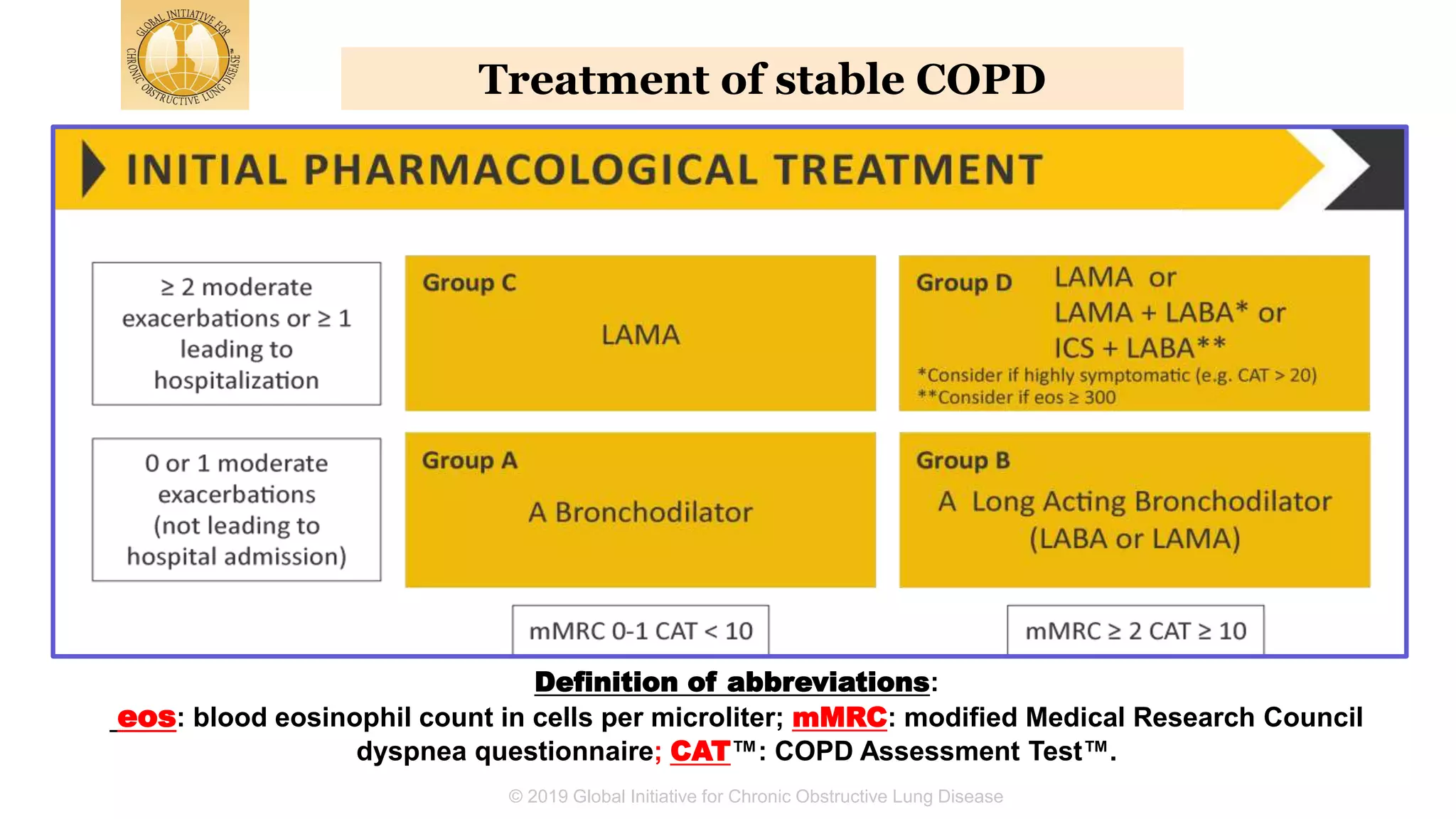
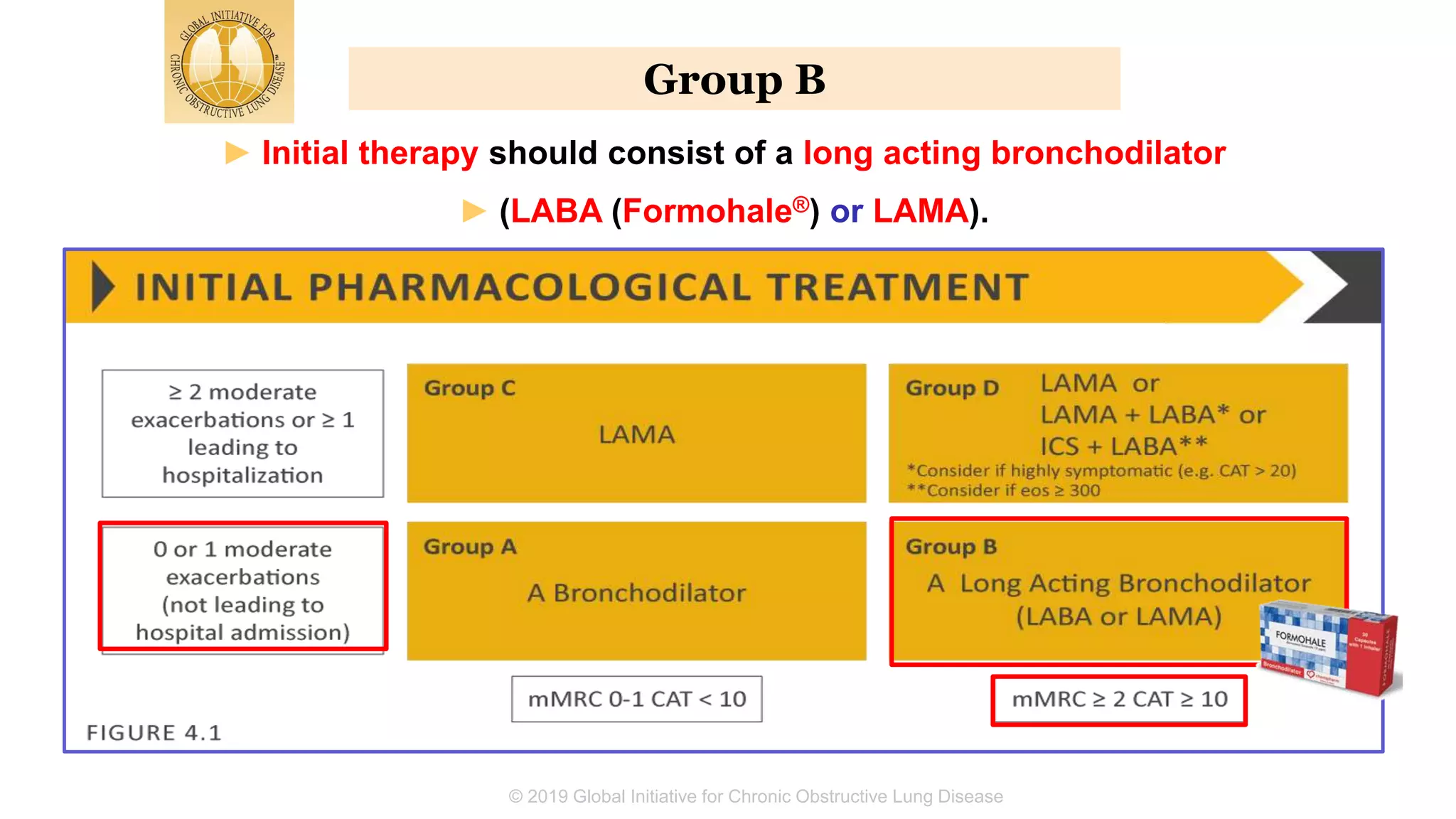
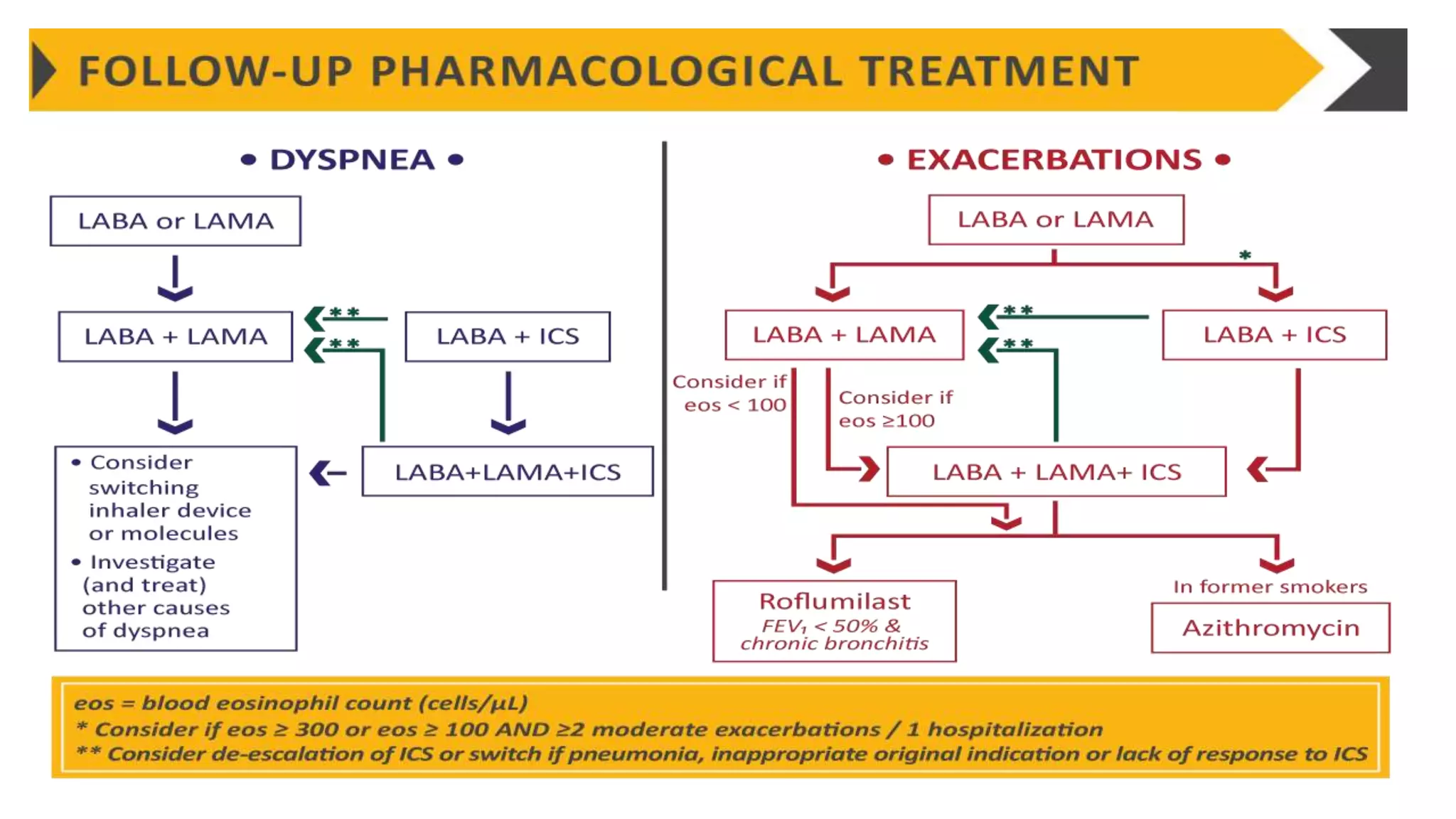
The document summarizes updates from the 2019 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines. It defines COPD and risk factors, outlines methods for diagnosis and assessment using spirometry, CAT and mMRC scales. Treatment approaches are discussed including bronchodilators, inhaled corticosteroids, and new biomarkers like blood eosinophil counts to predict treatment responses. Treatment algorithms are provided for managing stable COPD based on symptoms and exacerbation risks.