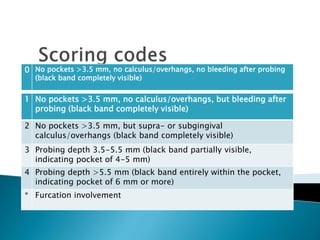
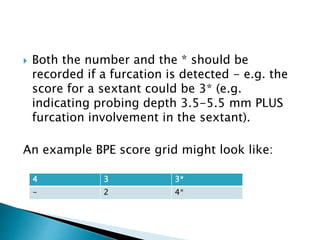
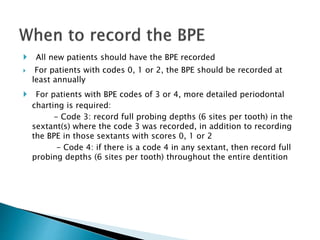
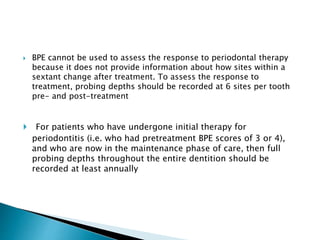
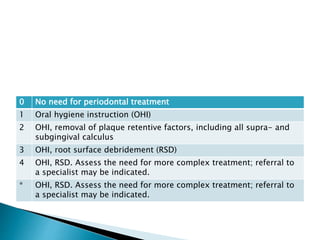
The document discusses the Basic Periodontal Examination (BPE), a screening tool used to assess periodontal disease levels and treatment needs. The BPE divides the mouth into sextants and codes pockets and furcations from 0-4 based on probing depth. A score of 3 or 4 indicates need for detailed charting or possible specialist referral. The BPE is useful for screening and monitoring but not assessing treatment response. Interpretation depends on individual factors, and radiographs are typically needed with scores of 3 or 4.