UPDATE ON BASICLIFE
SUPPORT
BLS FOR HEALTHCARE PROVIDERS
DR THULASI DEVI RAJU
Basic Life Support Training Manual ,2nd Edition 2023
2.
TOP MESSAGES
• EARLYRECOGNITION OF CARDIAC
ARREST
• ALERT EMS/ 999
• EARLY HIGH QUALITY CPR
• EARLY AED USAGE
3.
Chain of survival
Thekey observations are
unresponsiveness and not
breathing normally
Defibrillation within 3–5 mins of
collapse produce survival rates
50–70%.
Open Airway
Head tilt-chinlift
Head tilt: place one hand on the
forehead and not the eyes, to tilt
the head back
Chin lift: place fingers of the
other hand on the bony part and
not the soft tissue of the jaw, to
lift the chin
High quality CPR
-Site: middle chest, lower half of sternum
- Rate: 100 to 120 compressions per minute
- Depth: at least 5 cm and not greater than 6 cm
- Complete recoil of the chest
- Minimize interruption on chest compression
- Compression to ventilation ratio 30:2
- Ventilate adequately, each breath delivered over 1 second
with visible chest rise
14.
Figure 6 :Two hands technique
(E-C clamp technique)
Figure 5 : One hand technique
(E-C clamp technique)
• Each breath should be given over 1 second inspiratory
• No BVM, CPR only
BVM VENTILATION
16.
• Once AEDor Defib machine available : Attach
machine and check rhythm , shockable/ non
shockable
17.
AED, Defibrillator ARRIVES
SHOCKABLERHYTHM?
YES NO
Give 1 shock
Resume CPR For 5 cycles
Resume CPR For 5 cycles
and CHECK RHYTHM ;
Cont. till ALS Provider take over, victims start to move
When to stopCPR
1) Victim recovers with normal breathing
2) HCW is exhausted
3) Assistance arrives to take over CPR
4) Safety of provider can no longer be sufficiently assured
5) Obvious mortal injury or irreversible death
6) Asystole for more than 20 minutes despite ongoing BLS in
absence of reversible cause
SIGNS OF RECOVERY :
- WAKING UP/ MOVING/OPENING EYES/ NORMAL BREATHING
• If youare uncomfortable with intubation techniques
required and ventilation is adequate
• If patient’s condition improves during intubation attempts
• If respiratory arrest is reversible with drugs
• If patient has a deformity of the airway or neck but
stable
• If patient has a DNR order
Guidelines on when NOT to intubate
25.
TAKE AWAY MESSAGE
•Recognise and start early high quality
CPR
• Minimise interuptions during CPR
• Early AED usage
• Intubate if skillful and decide if really in
need
• Suction <10sec
• Epinephrine during the third CPR cycle,
and every 3-5 min afterwards
26.
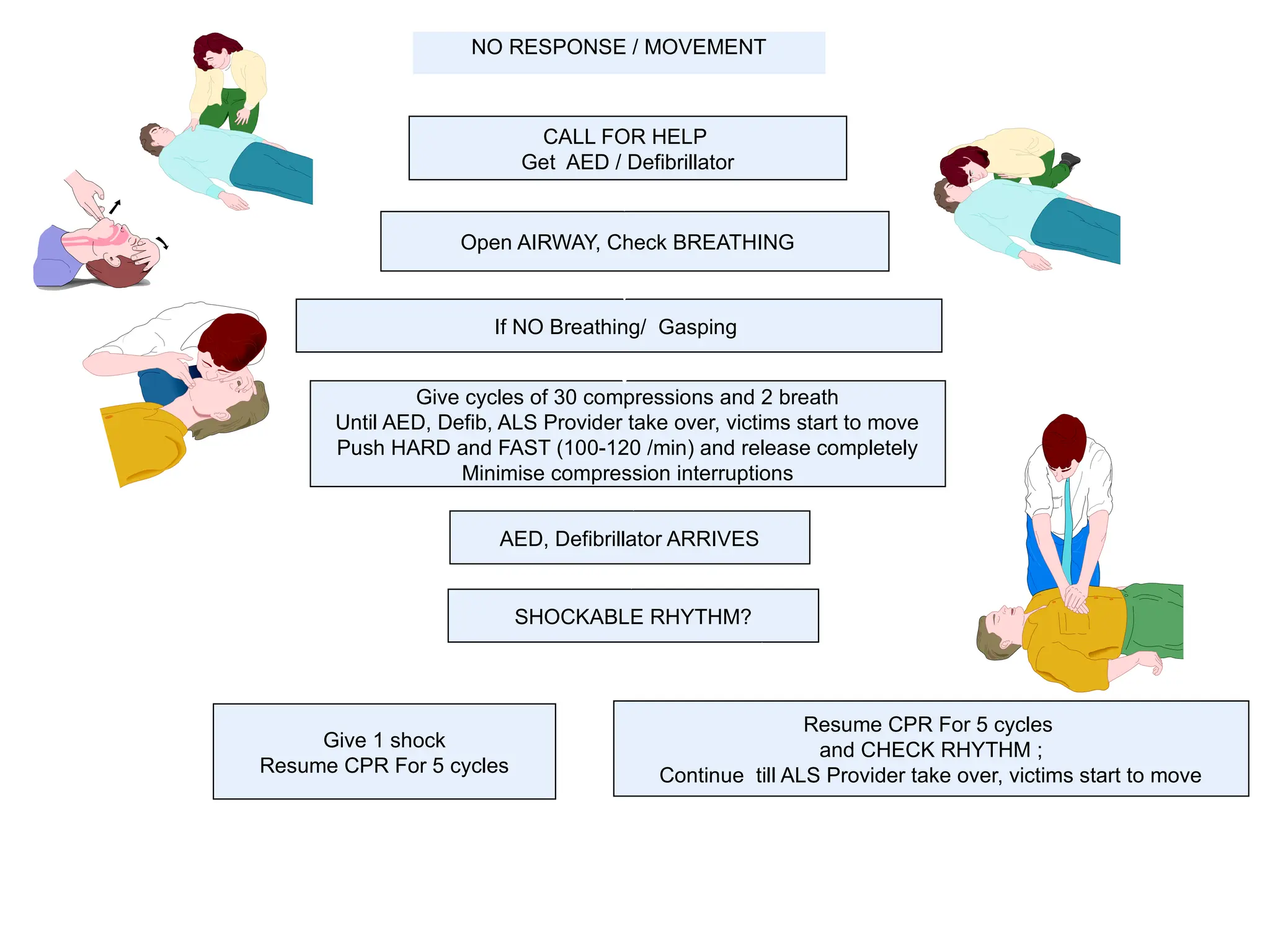
NO RESPONSE /MOVEMENT
CALL FOR HELP
Get AED / Defibrillator
Open AIRWAY, Check BREATHING
If NO Breathing/ Gasping
Give cycles of 30 compressions and 2 breath
Until AED, Defib, ALS Provider take over, victims start to move
Push HARD and FAST (100-120 /min) and release completely
Minimise compression interruptions
AED, Defibrillator ARRIVES
SHOCKABLE RHYTHM?
Give 1 shock
Resume CPR For 5 cycles
Resume CPR For 5 cycles
and CHECK RHYTHM ;
Continue till ALS Provider take over, victims start to move
YES NO
28.
Adult Foreign BodyAirway Obstruction
• Definition: severe difficulty in
breathing because of a constricted or
obstructed throat or a lack of air
29.
Recognize FBAO
• Witnessepisode
• Coughing or choking, gagging,
stridor
• Sudden onset respiratory distress
• Recent history of playing with or
eating small objects
• Universal sign
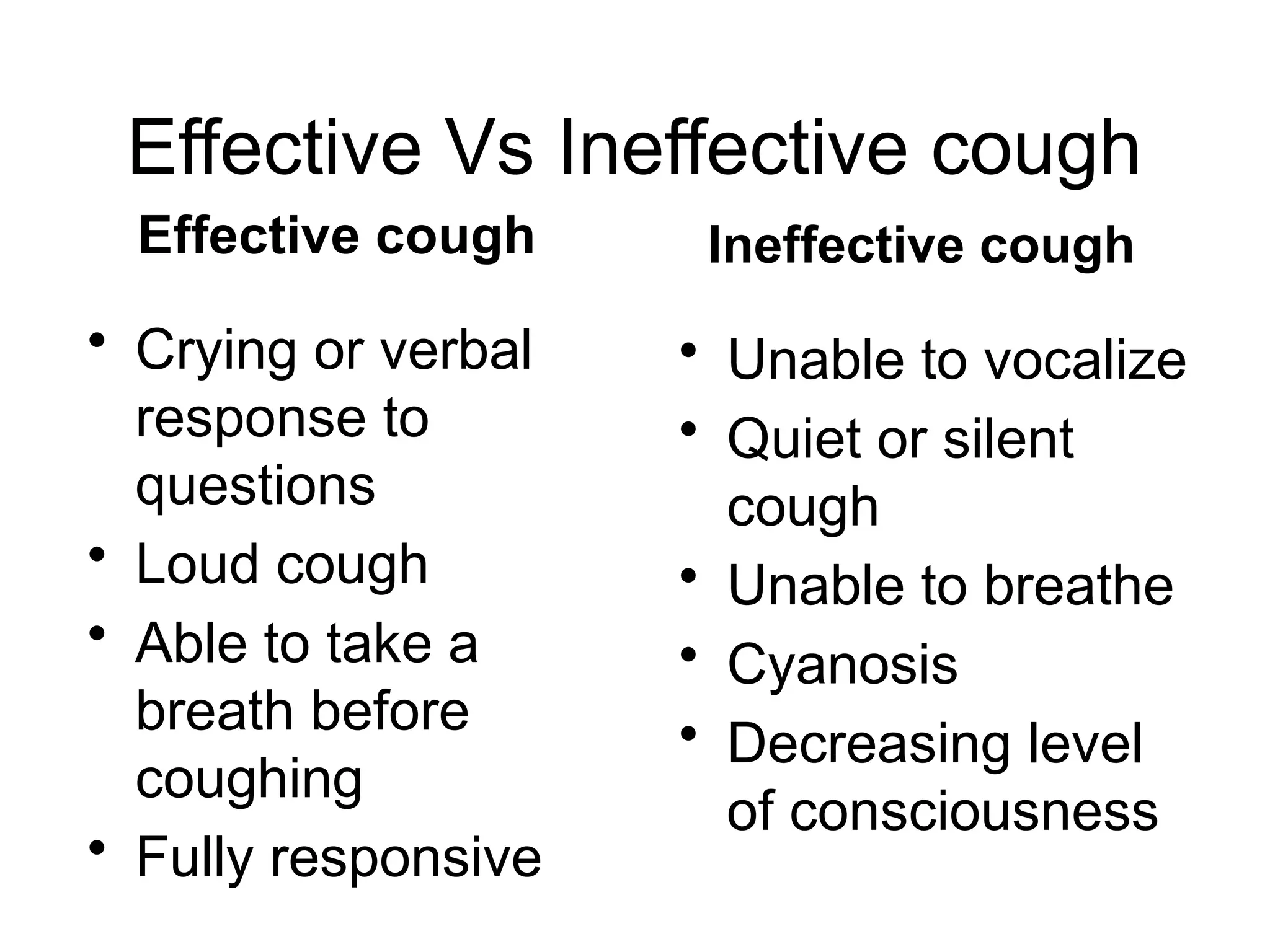
Effective Vs Ineffectivecough
Effective cough
• Crying or verbal
response to
questions
• Loud cough
• Able to take a
breath before
coughing
• Fully responsive
Ineffective cough
• Unable to vocalize
• Quiet or silent
cough
• Unable to breathe
• Cyanosis
• Decreasing level
of consciousness
32.
If cough isineffective, in conscious patient, give 5 back
blows following with 5 abdomen thrust/chest thrust
#1 SELAMAT PG KPD DR SURAIHAN, MOS, MAS DAN NURSES2. SAYA, DR THULASI AKAN MENYAMPAIKAN SEDIKIT REFRESHER ON BLS. I WILL BE USING BOTH MALAY AND ENGLISH TO ENSURE BETTER UNDERSTANDING ON THE TOPIC. THIS SLIDES ARE BASED ON BLS TRAINING MANUAL 2ND EDITION OF 2023. LATER ON , WE WILL HAVE PRACTICAL PART TO DO HANDS ON.
#2 THE TOP MESSAGE ATAUPUN PERKARA YG PALING DISTRESSKAN DLM MANUAL ADALAH SAMA SEPERTI SEBELUM INI
#3 the chain of survival summarizes the links for a successful resuscitation.
Early recognition and call for help - recognise chest pain earlier before pt collapses due to MI. If cardiac arrest happen, faster initiate ERS - emergency response System (ERS)- how to recognise earlier- the key observations are not responsive, not breathing and no pulse
- if already collapse- then start CPR immediately without wasting time, because within 4 minutes without oxygen, brain cells start to die req help and ask for AED, all done while initiating CPR (chest compression together with ventilation)
- once AED arrive, utilise it as early as possible, because studies show higher rate of survival with earlier AED usage
- Early advanced life support and post-resuscitation care to improve survival.
#4 This is the sequence of steps for the initial assessment and treatment of the unresponsive victim wherenby the mnemonics of drs abcd.
danger, response, shount and send, airway, breathing, circulation/cpr, defib
make sure its safe to help
check the vistim to response
shout for help and AED
open airway
assess breathing- not more than 10 sec, agonal breath or no breathing..
strat compression - high quality
once AED is there, assess for the need for shock
#5 Make sure you, the victim and any bystanders are safe
• Wear PPE (gloves, apron, mask) if available.
• Look out for blood spills, sharps, electric wires, unsteady beds, trolley.
#6 Check the victim for a response
a. Gently tap his shoulders/collarbone and ask loudly:
i. “Are you OK?”.
ii. If no response proceed to next step (Shout for Help)
b. If he responds, leave him in the position in which you find him, provided there is no further danger. Get help if needed and re-asses regularly.
#7 Shout for help/activate Emergency Response System(ERS)
• If alone, call for help VIA HANDS FREE OPTION- LIKE CALL IN SPEAKER PHONE while assessing for breathing and pulse without leaving the person.
- send somebody to get AED
#8 Open The Airway
a. Head tilt chin lift
• Place your hand on the forehead. Gently tilt the head back and with your fingertips under the point of the victim's chin, lift the chin to open the airway.
#9 b. Jaw thrust- if suspected cervical injury
• Use index and middle fingers to physically push the posterior aspects of the mandible upwards while your thumbs push down on the chin to open the mouth.
#10 • Check pulse simultaneously with checking for breathing. Do not pause more than 10 seconds to check for breathing and pulse.
#12 Start Chest Compressions
a. Place the heel of one hand in the centre of the victim’s chest at the lower half of the sternum.
b. Place the heel of your other hand on top of the first hand
c. Interlock the fingers of your hands and ensure that pressure is not applied over the victim’s ribs
d. Keep your arms straight
e. Position your shoulders vertically above the victim’s chest and press down on the sternum with high quality CPR
Switched the person applying chest compression every 5 cycles or 2 minutes to avoid fatigue.
b. Optimal chest compression are best delivered with the patient on a firm surface:
#13 High quality CPR
• Rate: 100 to 120 compressions per minute
• Depth: at least 5 cm and not greater than 6 cm (injuries are more common when compression depth is greater than 6 cm).
• Complete Recoil of the chest (to allow adequate perfusion to heart muscle and fill chambers during diastole)
- Do not lean on the chest.
• Minimize interruption on chest compression
- Delivery of rescue breaths, shocks, ventilations and rhythm analysis lead to
pauses in chest compression
- Pre-and post-shock pauses of less than 10s
1 person CPR, anotehr person give ventilation 1 in 5-6 sec
#14 Bag-valve-mask (BVM) ventilation
• Position yourself directly above the victim’s head.
• Place the mask on the victim’s face, using the bridge of the nose as a guide for correct position.
• Use the E-C clamp technique to hold the mask in place while you lift the jaw to hold the airway open:
- perform head tilt.
- use the thumb and index finger of one hand to make a “C” on the side of the mask, pressing the edges of the mask to the face.
- use remaining fingers to tilt angles of the jaw (3 fingers form an “E”).
• Squeeze the bag to give breaths (1 second each) while watching for chest rise.
#16 Early defibrillation is an essential step in the chain of survival for victims of cardiac arrest.
Defibrillation should be on as soon as it is available in shockable rhythm.
Before attach the pad, make sure shave if too hairy, the area in concern is dry, if pt has pacemaker, avoid attaching on top of it.
Adult pad can be used for those 8 years and above
#17 Once u have AED, turn on the power, chose pad (8 years and above- adult pad) and attach- one at right upper chest right below the clavicle and another one at the side of the heart’s apex.
If a shock is advised, deliver shock within 5 seconds
• Ensure that nobody is touching the victim with clear CHANT “I am clear, you are clear, everyone is clear…”. Make sure no free flow oxygen at the site.
• Push shock button as directed (fully automatic AEDs will deliver the shock automatically)
• Immediately restart CPR at the compressions:ventilation ratio of 30:2.
• Continue as directed by the voice/visual prompts.
If no shock is advised, continue CPR as directed by the voice/visual prompts.
#19 Reassessment
After every 5 cycles or 2 minutes of CPR, HCP shall check for normal breathing, less than 10 sec
#21 If you are certain the victim is breathing normally but is still unresponsive, place the victim in the recovery
position.
• Remove the victim’s glasses, if worn.
• Kneel beside the victim and make sure that both his legs are straight.
• Place the arm nearest to you at right angles to his body, elbow bent with the hand palm-up.
• Bring the far arm across the chest, and hold the back of the hand against the victim’s cheek nearest to you.
• With your other hand, grasp the far leg just above the knee and pull it up, keeping the foot on the ground.
• Keeping his hand pressed against his cheek, pull on the far leg to roll the victim towards you on to his side.
• Adjust the upper leg so that both the hip and knees are bent at right angles.
• Tilt the head back to make sure that the airway remains open.
• If necessary, adjust the hand under the cheek to keep the head tilted and facing downwards to allow liquid material to drain from the mouth.
• Check breathing regularly.
Be prepared to restart CPR immediately if the victim deteriorates or stops breathing normally
#22 A bit on airway- The basic airway adjuncts are oropharngeal and nasopharngeal airway
OPA- use in unresponsive (no cough/gag), angle of mouth to angle of jaw
NPA- can use in concious pt, not in facial trauma, tip of the nose to ear tragus
Laryngeal mask airway- alternative for intubation, cannot prevent aspiration, are various sizes available. - rescue breath
During CPR, the chest compression to ventilation rate for adults is 30:2.
• If advanced airway is placed, do not interrupt chest compressions for breaths. Give one breath every 6 seconds with continuous chest compressions once advanced airway is introduced. And suction attempt should be less than 10sec
#24
Early epinephrine found to have association with ROCS but not survival
For patients with shockable rhythm, defibrillation and CPR is prioritize initially and giving epinephrine if initial attempts with CPR and defibrillation
are not successful.
GIve epi during the thrid cpr cycle, then every 3-5 min aftr
• 1.0 mg (1:10,000) IV/IO or 1 ampule (1:1,000) in 10ml of normal saline
#26 DRSabcd
danger
response
shout for help
airway
breathing
circulation
defib
#30 encourage coughing until expoel FB, and then until improve
#31 No finger sweep unless foreign body visible
If cough is effective, encourage the victims to cough until the obstruction is relieved
#32 If cough becomes ineffective give up to 5 back blows
• Give five sharp blows between the shoulder blades with the heel of your hand.
If back blows are ineffective give up to 5 abdomina l thrust s
• Clench your fist and place it between the umbilicus (navel) and the ribcage
• Grasp this hand with your other hand and pull sharply inwards and upwards
• Repeat up to five times
• If the obstruction is still not relieved, continue alternating fiv e back blows with five abdominal thrusts
If the obstruction is still not relieved, continue alternating five back blows with five abdominal thrusts
If patient deteriorates to become unconscious, HCW should begin CPR.
#33 WAER PROPER PPE, ESPECIALY N95 AND GOOGLES
NO OPEN AIRWAY AND BREATHING ASSESSMENT
NO MOUTH2MOUTH VENTILATIONJ
ENSURE GOOD SEAL WITH BVM, USE TWO HANDS CLAMP EC.. CPR GUYS STOP AND SQUEEZE THE BAG