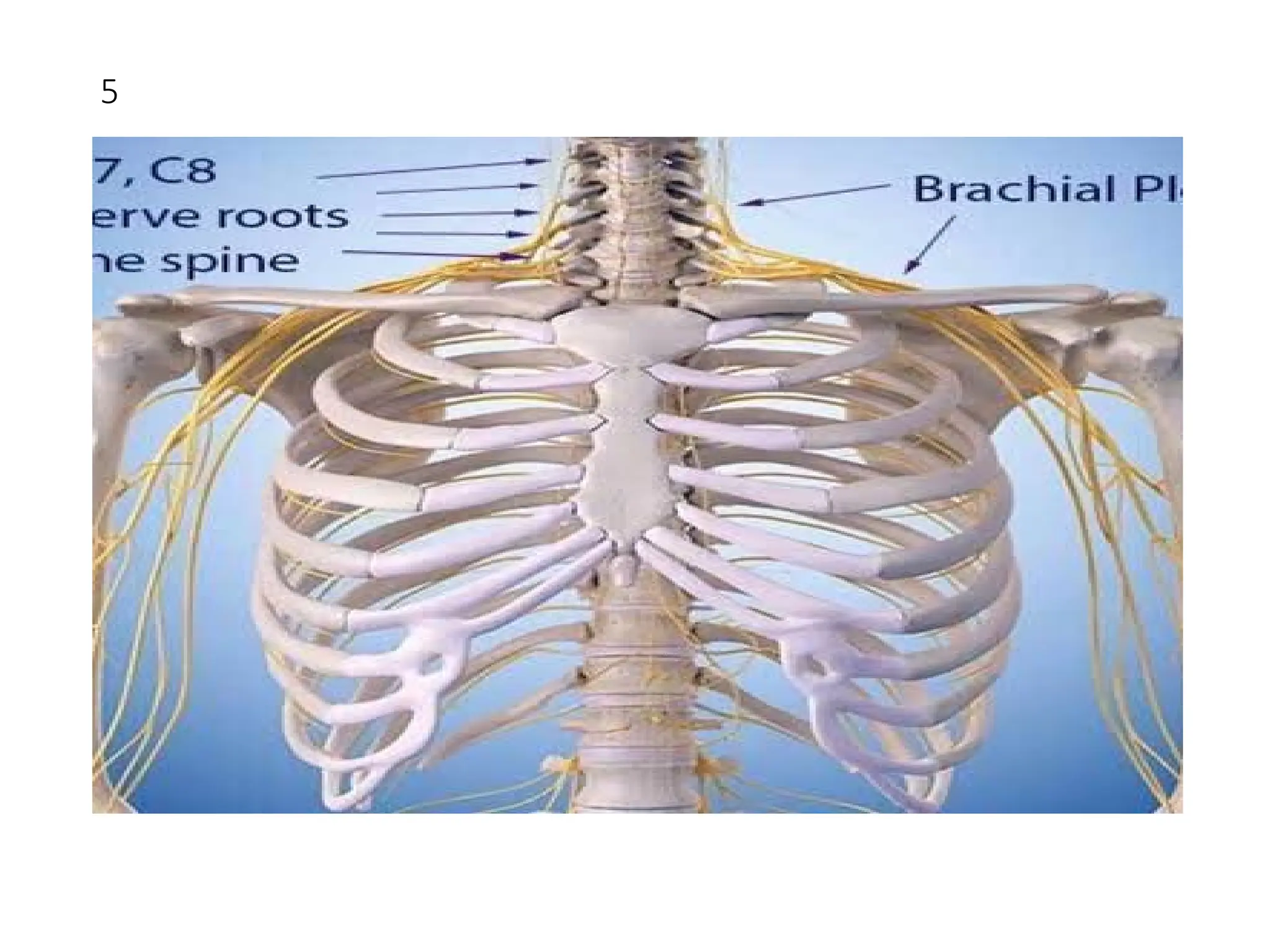
The document details the anatomy and functions of the axillary nerve, including its origins from the C5 and C6 spinal roots, its motor and sensory functions, and clinical relevance related to potential injuries. It outlines the nerve's role in innervating the deltoid and teres minor muscles, as well as the skin over the inferior deltoid area. Additionally, it discusses the implications of axillary nerve damage, treatment, and associated conditions like Erb's palsy.