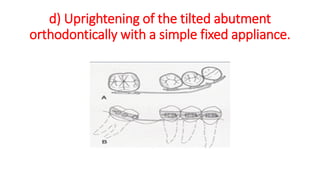
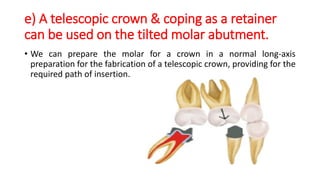
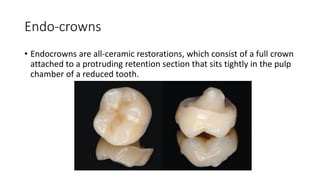
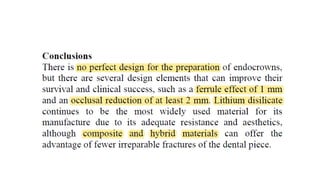
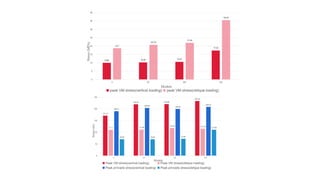
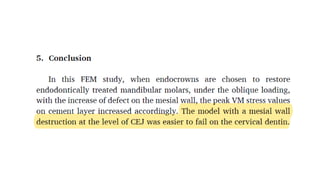
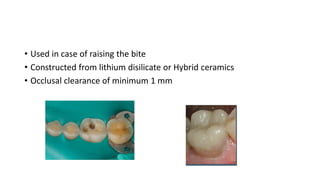
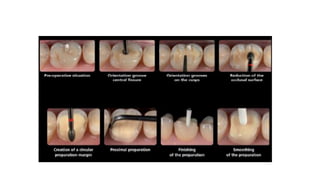
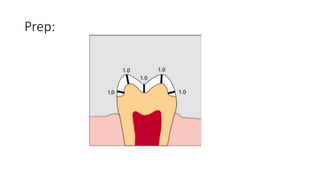
This document discusses atypical tooth preparations that are needed in certain clinical situations. It describes preparations needed for malaligned teeth, short teeth, mutilated teeth, periodontally compromised teeth, and endodontically treated teeth. For each situation, guidelines are provided for modifying the classic tooth preparation to address the specific problems presented while still providing adequate retention and resistance form. Endocrowns are also discussed as an alternative treatment for teeth with complete loss of the clinical crown where traditional post-and-core rehabilitation is not possible.