cardiac rhythm disorders in newborns
•Download as PPTX, PDF•
0 likes•1,459 views

Arrythmias in newborns

Recommended
More Related Content
What's hot
What's hot (20)
Similar to cardiac rhythm disorders in newborns
Similar to cardiac rhythm disorders in newborns (20)
More from Dr Praman Kushwah
More from Dr Praman Kushwah (20)
Recently uploaded
Recently uploaded (20)
cardiac rhythm disorders in newborns
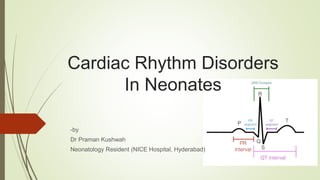
- 1. Cardiac Rhythm Disorders In Neonates -by Dr Praman Kushwah Neonatology Resident (NICE Hospital, Hyderabad)
- 2. 1. Reading an ECG 2. Normal Sinus Rhythm and Sinus Node Dysfunction 3. Sinus Arrhythmias 4. Tachyarrhythmias 5. Ventricular Arrhythmias 6. Genetic Arrhythmia Syndromes
- 5. Lead II has the most positive deflection compared to leads I and III Lead III has the most positive deflection and lead I should be negative •Lead I has the most positive deflection. •Leads II and III are negative.
- 8. Width can be described as NARROW (< 0.12 seconds) or BROAD (> 0.12 seconds):
- 9. ST-elevation is significant when it is greater than 1 mm (1 small square) in 2 or more contiguous limb leads or >2mm in 2 or more chest leads ST depression ≥ 0.5 mm in ≥ 2 contiguous leads indicates myocardial ischaemia
- 11. Normal Sinus Rhythm and Sinus Node Dysfunction Sinus node small, epicardial structure, at the posterior junction of the superior vena cava and right atrium. Balance of sympathetic and parasympathetic inputs determines the underlying heart rate at any given moment With normal cardiac anatomy, sinus bradycardia or sinus tachycardia are usually physiologic findings in newborns, the resting heart rate is typically 90 and 160 bpm, with intermittent decreases to as low as 70 bpm during rest or sleep
- 12. Sinus bradycardia <60 bpm (valid for infants and childrens) Generally physiologic Can be secondary to increased vagal tone Increased intracranial pressure, an acute abdominal process (e.g., necrotizing enterocolitis), suctioning of an endotracheal tube, gastric reflux, apnea of prematurity, or medications
- 13. Evaluation 1. Electrocardiogram (ECG) to evaluate for atrioventricular (AV) block any cardiac channelopathy 24-hour cardio scan monitor (Holter) to evaluate the infant’s heart rate variability Rarely used - a vagal nerve antagonist Atropine administration Increased HR bradycardia is secondary to vagotonia minimal or no heart rate increase primary sinus node dysfunction.
- 14. Treatment Rarely required Cases of episodic bradycardia to be evaluated. If no hemodynamic compromise no intervention If persistent hemodynamically significant Very rare, but pacemaker may be placed
- 15. Sinus tachycardia sinus rate above 160-180 bpm physiologic response to anemia, hyperthyroidism, fever, agitation, infection, or medications rarely - primary cardiac etiology ( cause leading to myocarditis). important to differiantiate from supraventricular tachycardia (SVT).
- 16. findings that suggest a pathologic mechanism 1. The lack of heart rate variability 2. Abnormal P-wave morphology or axis (normally upright in leads I and aVF) on ECG 3. Prolongation of PR interval 4. Very rapid increases or decreases in heart rate 5. Abnormal cardiac function on echocardiogram
- 17. Evaluation ECG to rule out pathologic arrhythmia 24-hour Holter Treatment treat the underlying cause Note - Neonates with high resting heart rates generally do not require any treatment but should be closely evaluated to make sure they do not have a secondary cause such as infection or anemia
- 18. Sinus Arrhythmia a/k/a respiratory sinus arrhythmia phasic variations in heart rate seen with an increase in heart rate during inspiration and a decrease in heart rate with expiration by the so-called Bainbridge reflex (baroreceptor reflex) Appropriate ECG interpretation is helpful if the diagnosis is in question variation in the rate no change in the appearance of the P-wave morphology or axis no treatment or follow-up required.
- 20. Arrhythmias Arrhythmias in the neonatal period are not uncommon A normal heart or in with structural heart disease incidence of neonatal arrhythmia is 1%–5% in all neonates Congenital heart disease (CHD) not only affects the anatomical defect but also causes electrical changes, that induce various arrhythmias. Surgical correction may also be related to the cause of arrhythmia in patients with CHD.
- 21. Classification Classified as either benign or non benign. Benign arrhythmias sinus arrhythmia, premature atrial contraction (PAC), premature ventricular contraction (PVC), and junctional rhythm; these arrhythmias have no clinical significance and do not need therapy. Non-benign arrhythmias Supraventricular tachycardia (SVT), ventricular tachycardia (VT), atrioventricular (AV) conduction abnormalities, and genetic arrhythmias such as congenital long-QT syndrome (LQTS)
- 22. Tachyarrhythmias I. Atrial Tachycardia II. Reentrant Supraventricular Tachycardia
- 23. I. Atrial Tachycardia 1. Premature Atrial Contractions 2. Atrial Ectopic Tachycardia 3. Atrial Flutter 4. Atrial Fibrillation 5. Chaotic atrial tachycardia
- 24. 1. Premature Atrial Contractions Common in the neonatal period and manifest as irregular heartbeats. Types Of PAC A premature P wave superimposed on the previous T wave can cause deformation of the T wave. Nonconduction of PACs can sometimes occur and be misdiagnosed as sinus bradycardia in neonatal intensive care units. the aberrant conduction of PACs causes a different QRS morphology Isolated PACs in neonates are associated with electrolyte abnormalities, hypoglycemia, hypoxia, and hyperthyroidism. PACs are generally benign and usually do not need treatment
- 25. Premature Atrial Contraction Conducted Not conducted Aberrantly conducted • Usually happens • P wave followed by normal looking QRS wave • a/k/a “blocked” PAC • AV node or bundle of His is refractory • P wave not followed by QRS • clinically bradycardia • If either the right or left bundle branch is refractory • P wave will be followed by a wide QRS (aberrant ventricular conduction).
- 27. 2. Atrial Ectopic Tachycardia Three or more consecutive PACs and rate >120 beats per minute increased automaticity of atrial myocardium (abnormal firing foci) Direct stimulation - arterial catheter with the tip in the atrium On ecg – different P-wave morphology Evaluation ECG and Holter monitoring 2d echo to rule out CHD Electrolyte Disturbances - should be corrected
- 28. Treatment Medications beta blockers (propranolol), sodium channel blockers (flecainide) class III antiarrhythmic medications (sotalol, amiodarone). Spontaneous resolution - in the first 6 months refractory atrial tachycardia Cardiac - Radiofrequency ablation (RFA)
- 29. 3. Atrial Flutter a/k/a atrial reentry tachycardia. the circuit for reentry is myocardium around tricuspid valve typical atrial rate b/w 300 and 600 beats per minute ventricular rate much less decremental properties of the AV node conduction to the ventricles is in ratio 2 : 1, 3 : 1, or 4 : 1 Evalution ECG - continuous sawtooth pattern (adenosine administerd sometimes for easy identification of the sawtooth pattern P waves are masked by QRS complexes or T waves.
- 30. Treatment Initial treatment - synchronized electrical cardioversion 0.5-2 J/kg Conservative - antiarrhythmic medications long term antiarrhythmic medications (propranolol or digoxin) underlying atrial dilation recurrent atrial flutter structural heart disease
- 31. 4. Atrial Fibrillation Exceptionally rare dysrhythmia A/w – severe structural congenital heart disease (such as Ebstein anomaly of the tricuspid valve) an accessory pathway (Wolff-Parkinson- White) cardiac channelopathies ECG - Irregular tachycardia with disorganized atrial activity Distinguish from Chaotic atrial tachycardia (or multifocal atrial tachycardia) Treatment – synchronized cardioversion Pediatric cardiology consultation should be obtained
- 32. 5. Chaotic atrial tachycardia a/k/a multifocal atrial tachycardia ECG - irregular tachycardia with disorganized atrial activity (Same as Afib) Occur in short bursts with sinus beats interspersed May or may not respond to cardioversion medical treatment with antiarrhythmic medications needed (alone or in combinations) beta blockers flecainide, sotalol amiodarone,
- 34. Most common form of SVT in neonates Mechanism – two distinct conducting pathways linked around an area of nonconducting tissue. Failure to conduct in one of these pathways (block) causes the impulse to turn around in the other pathway, creating an electrical loop that causes tachycardia reentrant mechanisms Pathways 1. Accessory pathway (m/c) (Manifest OR Concealed) 2. Through atrioventricular node a/k/a atrioventricular nodal reentry tachycardia
- 35. Accessory Pathway accessory pathway additional conduction pathway Conduction Bidirectional Unidirectional – Antegrade Atria to ventricle OR Retrograde Ventricle to atria Retrograde conducting accessory pathway a/k/a concealed accessory pathway baseline ECG will appear normal Antegrade conducting cessory pathway manifest accessory pathway preexcitation on the baseline ECG (Wolff-Parkinson- White).
- 37. Wolff-Parkinson- White Antegrade conducting acessory pathway ECG - delta wave short PR interval and widened QRS complex normal physiologic delay does not exist with accessory pathway and ventricular myocardium activates before it would normally be activated resulting in a delta wave on the ECG A/w underlying structural heart disease (most commonly Ebstein anomaly) atrial fibrillation as wide complex tachycardia or sudden cardiac death Adenosine should be used in a very controlled environment digoxin relatively contraindicated
- 40. Presentation rapid increase in heart rate (Any Sinus rate > 220 bpm – possibility) Ventricular rates - 200 -300 bpm Narrow complex tachycardia on ECG. Some times - wide complex tachycardia (a/w left bundle branch block) Persistent tachycardia can cause depressed myocardial function a/w generalized symptoms - poor feeding and irritability tachycardia with preexcitation on ECG – s/o WPW
- 42. Treatment Consider - hemodynamically stable or unstable Anticipate - intubation, cardioversion, and resuscitation adenosine or direct current cardioversion. intravenous pressors and even ECMO can be needed cardioversion - 0.5 and 1 joule per kilogram (larger doses may be required) If QRS complex generating a pulse - synchronized cardioversion
- 43. First line – vagal stimulation small bag or glove filled with ice over the entire face for 10-15 seconds) Holding a child upside down Gagging, ocular pressure, and anal stimulation should be avoided adenosine administration IV adenosine (dose is 0.1 mg/kg per dose, if the arrhythmia persists, then 0.2 mg/kg per dose) rapid IV push followed by a 5-10 cc bolus normal saline IV amiodarone refractory cases of SVT (as per pediatric cardiologist) Second-line sotalol, flecainide, or amiodarone (only under pediatric cardiologist recommendation)
- 47. Long term – 60%-80% resolve spontaneously within the first year of life Beta blockers (propranolol 1 mg/ kg /dose Q 6 H) cardiac catheterization and ablation drug-refractory tachycardias Digoxin (fetal tachycardias 4-5 μg/kg per dose given twice a day)
- 48. Junctional reciprocating tachycardia (PJRT) Tachycardia present immediately after birth P waves before each QRS complex, which may be mistaken for sinus rhythm deeply negative clearly visible P waves in the inferior leads II, III, and aVF tachycardia-induced cardiomyopathy if left untreated spontaneous termination or spontaneous reinitiation Treatment antiarrhythmics. Flecainide - treatment of choice an ablation if does not resolve
- 50. Junctional Ectopic Tachycardia Increased automaticity is focus of tachycardia present in bundle of His (most commonly) proximal bundle branches (very rarely) On ECG - tachycardia with no association b/w P waves & QRS complexes (VA dissociation), Ventricular(narrow QRS) rate being faster than the atrial rate.
- 51. Acquired JET Commonly after cardiac surgeries for CHDs Mechanism - swelling/edema, electrolyte imbalances, catecholamine surges, vasopressors resolves within 3-5 days after surgical repair heart rate in range of 150-170 hemodynamically stable no specific treatment hemodynamically unstable Treat fever and/or cool the patient. Decrease/wean all catecholamines. Initiate atrial pacing at rates faster than the JET rate to restore AV synchrony. Administer amiodarone or procainamide intravenously for at least 48 hours.
- 52. Congenital JET Rare life-threatening tachycardia in fetuses, neonates, and infants less than 6 months tachycardia-induced cardiomyopathy mortality rate of greater than 50% Usually not respond to any form of intervention Conservative remove additional catecholamines initiate amiodarone or procainamide Adenosine - minimal response to tachycardia, used for AV disassociation
- 54. Ventricular Arrhythmias 1. Premature ventricular contractions 2. Ventricular tachycardia (VT)
- 55. Premature ventricular contractions Relatively uncommon compared with PACs On ECG No preceding P wave different morphology of premature QRS complex Common causes CHD, cardiomyopathy, inflammatory myocardial disease, metabolic disease, electrolyte disturbance and LQTS frequent PVCs are defined as >60 beats/hr in a child Causes of frequent PVCs immaturity of cardiac conduction tissue and autonomic nerve system Isolated PVCs usually resolve spontaneously, and no treatment is required a normal heart asymptomatic frequent PVCs in newborns have a good long-term prognosis
- 57. Ventricular tachycardia (VT) When rhythm disturbance is below the bifurcation of bundle of His Typical - wide complex rhythm (QRS > 80 ms) Ventricular tachycardia rhythm – Bening Form idioventricular rhythm (accelerated ventricular rhythm) rate no more than 20% faster than the underlying sinus rate patient is asymptomatic and hemodynamically stable requires no intervention
- 58. Structurally normal hearts Automatic focus is cause the outflow tract (RV Outflow is m/c) or one of the fascicles in the left ventricle Cardiac tumors or myocardial hamartomas rare, causes extremely difficult to control with medications May require surgical resection. poor ventricular function myocarditis / structural cardiac disease
- 60. Treatment Idioventricular rhythm and Asymptomatic no therapy required normal ventricular function beta blockers (propranolol) flecainide, sotalol or amiodarone Decreased ventricular function rapid control - important IV Amiodarone or sotalol
- 61. Long-term therapy Many resolve spontaneously (in first several months) refractory tachycardia Radiofrequency ablation Hamartoma or tumor surgical excision poor ventricular function Implantable cardioverter-defibrillator (ICD) therapy
- 62. Genetic Arrhythmia Syndromes Inherited disorders causing cardiac dysrhythmias and even death Channelopathies (m/c) Disruptions in myocardial ion channels (e.g., sodium, potassium, calcium) altered electrical depolarization and repolarization atrial and/or ventricular arrhythmias. Examples of channelopathies long QT syndrome (major culprit) catecholaminergic polymorphic ventricular tachycardia (CPVT), Brugada syndrome short QT syndrome
- 63. Long QT Syndrome ECG - prolongation of the corrected QT interval (QTc) torsades de pointes - lethal form of cardiac arrhythmias polymorphic ventricular tachyarrhythmia leading ventricular fibrillation sudden death Pathophysiology reduced cardiac output during the arrhythmia brain hypoperfusion true seizures (recurrent syncopal episodes or seizure episodes )
- 64. Inherited Types are LQT1, LQT2, and LQT3 syndromes Other causes Drug Induced (methadone, erythromycin, albuterol, etc.) Can cause lifethreatening ventricular arrhythmias (esp. if QTc is >500 msec) Electrolyte disturbances (hypocalcemia, hypokalemia)
- 65. LQTS presentation incidentally on an ECG pseudo or pure AV block (QT interval must be evaluated) As ventricular arrhythmias Sudden death (SIDS) Torsades de pointes (LQTS should be suspected)
- 66. Evaluation Measured in leads II and V5 on the ECG If QTc intervals between 450 and 500 msec (Normal < 450 msec
- 67. Treatment avoid QTc prolonging medications Start nonselective beta blocker (typically nadolol or propranolol) Pediatric cardiologist consultation Pacing if AV block caused by LQTS Sympathectomy (new modality) Treatment of Torsades de Pointes Discontinue any potential offending drug. Avoid amiodarone Magnesium bolus and continuous infusion Isoproterenol can be used if magnesium is unsuccessful.
- 72. Supraventricular tachycardia (SVT), a tachyarrhythmia that originates proximal to the bundle of His, can occur in infants who have underlying congenital heart defects. Of the following, the most common congenital heart disease that predisposes to SVT is: A. Coarctation of the aorta. B. Ebstein anomaly of the tricuspid valve. C. Pulmonary atresia with intact ventricular septum. D. Tetralogy of Fallot. E. Total anomalous pulmonary venous return.
- 73. A term newborn has recurrent episodes of tachycardia that began at 12 hours of age. During one such episode, the heart rate is 280 beats/min. Electrocardiography reveals inverted P waves, most of which follow QRS complexes; normal QRS pattern; and P-R intervals that exceed R-P intervals. The infant is hemodynamically stable, has no echocardiographic evidence of congenital heart disease, and has no indwelling vascular catheters. Vagal maneuvers and intravenous adenosine are unsuccessful in restoring normal heart rhythm. Of the following, the next pharmacologic agent recommended, according to the algorithm for management of neonatal supraventricular tachycardia, is: A. Amiodarone. B. Digoxin. C. Esmolol. D. Procainamide. E. Propafenone
- 74. In neonatal cases of supraventricular tachycardia nonresponsive to a single pharmacologic agent, a combination of medications may be tried. Of the following, the combination of medications most successful in controlling refractory supraventricular tachycardias is: A. Amiodarone and propranolol. B. Digoxin and amiodarone. C. Digoxin and propranolol. D. Flecainide and amiodarone. E. Flecainide and sotalol.
- 75. Take Home Message Neonates can experience all forms of arrhythmias Atrial flutter common in newborns, treatment is synchronized cardioversion. supraventricular tachycardia IV adenosine is treatment of choice 60 – 80 % supraventricular tachycardias resolve by 1 year of age
- 76. THANK YOU