Associate Professor Ian Scott
Director
Internal Medicine & Clinical Epidemiology; Associate Professor of Medicine
Princess Alexandra Hospital; University of Queensland
Implementing American Heart Association Practice Standards for Inpatient ECG ...Allina Health
Implementing American Heart Association Practice Standards for Inpatient ECG Monitoring: An Interventional Study at Abbott Northwestern Hospital presented by Kristin Sandau, PhD, RN
Developing and implementing clinical standards for seven day servicesNHS Improving Quality
Celia Ingham Clark National Director: Reducing Premature Mortality. Slides from Celia's presentation from the 7 Day Services events West Midlands 11th June and East Midlands 12th June 2014
Implementing American Heart Association Practice Standards for Inpatient ECG ...Allina Health
Implementing American Heart Association Practice Standards for Inpatient ECG Monitoring: An Interventional Study at Abbott Northwestern Hospital presented by Kristin Sandau, PhD, RN
Developing and implementing clinical standards for seven day servicesNHS Improving Quality
Celia Ingham Clark National Director: Reducing Premature Mortality. Slides from Celia's presentation from the 7 Day Services events West Midlands 11th June and East Midlands 12th June 2014
Determinants of Fall Risk and Injury in Hispanic Elderly Living in El Paso Community
Guillermina Solis, PhD, RN, F/GNP
Vanessa Guerrero, RN
Mano y Corazón Binational Conference of Multicultural Health Care Solutions, El Paso, Texas, September 27-28, 2013
Dr David Maltz: The challenge of length of stayNuffield Trust
In this slideshow, Dr David Maltz, of The Oak Group, explores the challenge of length of stay and opportunities for improvement.
Dr Maltz spoke at the Nuffield Trust ‘Reducing the length of stay’ event in September 2014.
Providing actionable healthcare analytics at scale: Understanding improvement...Nuffield Trust
Thomas Woodcock, Improvement Science Fellow at Imperial College London, talks about the various measurement approaches and processes when working at large scale to assess care quality improvements.
Introduction of the NZ Health IT Plan enables better gout management - Reflections of an early adopter. Presented by Peter Gow, Counties Manukau DHB, at HINZ 2014, 12 November 2014, 11.37am, Plenary Room
Stopping over-medication of People with Learning Disabilities
(STOMPLD) 2016.
Reducing Inappropriate Psychotropic Drugs in People with a Learning Disability in General Practice and Hospitals in 2016.
Expediting Colonoscopy for Patients with + Faecal Occult Blood Test in a Publ...Cancer Institute NSW
Colon cancer is the commonest cancer in Australia. The Federal Gov. has recently accelerated the rollout of the National Bowel Cancer Screening Program to 2nd yearly after age 50 by 2018. We anticipate up to 1000 extra colonoscopies on the public system at NSLHD.
A device to convert any toilet at an outreach camp or a healthcare facility in to a smart biosensing toilet to screen and/or diagnose chronic kidney disease.
Predictors of MDT review and the impact on lung cancer survival for HNELHD re...Cancer Institute NSW
Review by a Multidisciplinary Team (MDT) has been shown to lead to increased rates of surgical resection, radiotherapy, chemotherapy and timeliness of care. Most recently, the Victorian lung cancer patterns of care study have found that MDT review is an independent predictor of lung cancer survival.
Dr Derek Thompson: Building a caring futureNuffield Trust
In this slideshow, Dr Derek Thompson, GP and Medical Director at Northumbria Healthcare Foundation Trust, on reducing the length of hospital stay and building a caring future.
Dr Thompson spoke at the Nuffield Trust ‘Reducing the length of stay’ event in September2014.
Determinants of Fall Risk and Injury in Hispanic Elderly Living in El Paso Community
Guillermina Solis, PhD, RN, F/GNP
Vanessa Guerrero, RN
Mano y Corazón Binational Conference of Multicultural Health Care Solutions, El Paso, Texas, September 27-28, 2013
Dr David Maltz: The challenge of length of stayNuffield Trust
In this slideshow, Dr David Maltz, of The Oak Group, explores the challenge of length of stay and opportunities for improvement.
Dr Maltz spoke at the Nuffield Trust ‘Reducing the length of stay’ event in September 2014.
Providing actionable healthcare analytics at scale: Understanding improvement...Nuffield Trust
Thomas Woodcock, Improvement Science Fellow at Imperial College London, talks about the various measurement approaches and processes when working at large scale to assess care quality improvements.
Introduction of the NZ Health IT Plan enables better gout management - Reflections of an early adopter. Presented by Peter Gow, Counties Manukau DHB, at HINZ 2014, 12 November 2014, 11.37am, Plenary Room
Stopping over-medication of People with Learning Disabilities
(STOMPLD) 2016.
Reducing Inappropriate Psychotropic Drugs in People with a Learning Disability in General Practice and Hospitals in 2016.
Expediting Colonoscopy for Patients with + Faecal Occult Blood Test in a Publ...Cancer Institute NSW
Colon cancer is the commonest cancer in Australia. The Federal Gov. has recently accelerated the rollout of the National Bowel Cancer Screening Program to 2nd yearly after age 50 by 2018. We anticipate up to 1000 extra colonoscopies on the public system at NSLHD.
A device to convert any toilet at an outreach camp or a healthcare facility in to a smart biosensing toilet to screen and/or diagnose chronic kidney disease.
Predictors of MDT review and the impact on lung cancer survival for HNELHD re...Cancer Institute NSW
Review by a Multidisciplinary Team (MDT) has been shown to lead to increased rates of surgical resection, radiotherapy, chemotherapy and timeliness of care. Most recently, the Victorian lung cancer patterns of care study have found that MDT review is an independent predictor of lung cancer survival.
Dr Derek Thompson: Building a caring futureNuffield Trust
In this slideshow, Dr Derek Thompson, GP and Medical Director at Northumbria Healthcare Foundation Trust, on reducing the length of hospital stay and building a caring future.
Dr Thompson spoke at the Nuffield Trust ‘Reducing the length of stay’ event in September2014.
For more information contact: Slideshare@marcusevans.com
Presentation delivered by Donna Medina, Regional Director,OSF Hospice and Homecare Foundation at the marcus evans Home Care Leadership Summit held on July 13 & 14 2015 in Palm Beach FL.
Population Health Management PHM MLCSU huddleMatthew Grek
Andi Orlowski (Director of The Health Economics Unit) give an overview of Population Health Management (PHM) to the Midlands and Lancashire Commissioning Support Unit Huddle, on 25 March 2021
• Implementing ACE in 100 aged care facilities
• Building relationships with aged care staff for improved patient outcomes
• Examining savings and delivering results
Speaker: Jacqueline Hewitt Clinical Nurse Consultant John Hunter Hospital, NSW
Jacquie White, Deputy Director of NHS England Long Term Conditions, Older People & End of Life Care and Dr Eileen Pepler, Academic, Researcher and Consultant in the Canadian Healthcare will discuss how NHS England work in chronic disease is being translated into a Canadian context.
An opportunity to hear how service redesign positively impacts on the patient experience and improves outcomes for both the patient and NHSScotland. Showcasing examples of changes to pathways of care in orthopaedics and community support for people with complex and chronic conditions.
Introduction to Supporting recovery in Primary Care using Proactive Framework...Innovation Agency
Presentation by Julia Reynolds, Associate Director for Transformation - Innovation Agency at the Supporting recovery in Primary Care using Proactive Frameworks for Long Term Conditions event on Thursday 15 September 2022.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Associate Professor Ian Scott - Princess Alexandra Hospital; University of Queensland
1. Impact of an acute ambulatory
care program on ED access and
patient flows
Ian Scott MBBS, FRACP, MHA
Director of Internal Medicine and Clinical Epidemiology, Princess Alexandra
Hospital
Co-chair, Statewide General Medicine Clinical Network
Associate Professor of Medicine, University of Queensland
Emergency Department Management Conference
Sydney
31/7/17
2. Challenges in Metro South HHS
• Ageing population
– 12% over 65 which will increase to 16% by 2026 with
high co-morbidity burden
• Increasing ED presentations
– ~5% increase per year to 2016
• Growth in acute inpatient admissions
outstripping population growth by > 5:1
• Almost half acute medical admissions spend
less than 48 hours in hospital
• Sub-optimal QEAT compliance rates (average
65% versus state target of 80%)
• Exit block with hospital occupancy rates >90%
– 1 in 14 hospital beds occupied by non-acute patients
• Unplanned readmissions (~ 20%)
• Bed demand increasing due to population
growth
– Population bed shortage >400, to 1200 by 2026
3. Maximising whole system flow
Reduce attendances
• Hospital avoidance
• Substitutive care
Reduce admissions
• Ambulatory care units
• MAPUs
• HITH
Streamline care
• Care and disposition
protocols
• Co-management
• Single point referrals
• Pull strategies
Reducing exit block
• Discharge
planning
• Stranded patient
programs
• Push strategies
Patient journey
Readmission reduction programs
5. Avoiding ED presentations
• Direct call line which provides GPs direct access to a general
physician on call who can provide expert opinion on patients
presenting to GPs with acute clinical syndromes
• Rapid Access to Consultative Expertise (RACE) consultant can advise
the GP whether to refer the patient to ED, AACU, Rapid Access
Clinics, HITH or Palliative Care
• Aim of the RACE call-line is to redirect patient referrals away from
ED if appropriate care can be delivered in alternative settings
• Up to 30% of GP referrals to ED can be managed via alternative
pathways
Dale et al. Emerg Med J 2003;20:178–83.
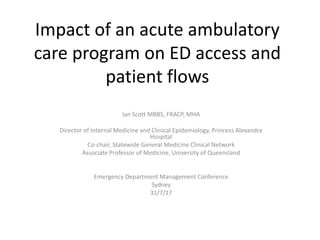
7. Expediting patient flow following ED
presentation
– The streams ‘overlap’ – very many can have reduced LOS
– Allocate early (Day 0) to teams skilled in that stream
0
50
100
150
200
250
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59
Length of stay (days)
Numberofpatients
Specialty - Clarity of specialty criteria
Early management plan
Minimal process delays
Short stay – manage to the hour
Maximise ambulatory care
Stranded patients
Identify and address causes of delay
Older, frail, multi-morbid
Early CGA
Minimise moves
Minimise deconditioning
Early assertive management
Minimally intrusive care
8. Expediting patient flow
30%
50% of demand –
Avoid downstream
longer than necessary stays
19%
1% of demand
Specialty cases
Single organ isease
Trauma
Mental health
0
100%
Cumulative ED demand
LOS
Sick frail, multi-
morbid patients
Short stay patients
< 48 hours
Very complex patients
9. Expediting decision-making and
patient flow within ED
• Real-time monitoring of ED caseload
– Identifying probable medical admissions
• Frequent ED rounding with general physicians
– Expediting care and disposition decisions
– Single patient vs batch processing
– Parallel vs linear processing
• Rapid response to requests for review/advice/admission
– Path of least resistance
– Navigates and negotiates the downstream path
• Assistance with undifferentiated clinical presentations
• Collaboration in developing standardised care protocols for common presentations
that minimise low value care which wastes time and resources
– 4Fs project (fits, feints, funny turns, falls)
– acute geriatric syndromes
PULL
strategies
Sullivan et al Aust Health Rev 2015
11. Expediting patient flow across the
ED-inpatient interface (EDII)
• Single point referral contact for requests for
advice/review/admission
• MASPER/CASPER
• ‘Take it and own it – the clock’s running’
• On-floor consultant for rapid review and decision-making for
admissions to non-critical care wards
• Physician supervised clinical decision units or transition units
• Redirect and fast track high-risk older, frail patients to purpose-
designed older patient care areas
– Acute frailty units; acute care of elderly (ACE) units
• Direct to ward admission pathways co-ordinated by general
medicine flow nurses
12. Avoiding in-patient admissions
• Redirect and fast track patients presenting to
ED into alternate non-inpatient services where
appropriate
– Acute ambulatory care units
– MAPU
– HITH
– Rapid access clinics
– Hospice care, interim care
– Targets all patients who ED would have admitted
as overnight stays but who are likely to have LOS
<48 hours
13. Acute ambulatory care units (AACU)
• Short stay medical unit (8am-8pm) that provides urgent assessment,
investigation, and management for patients with acute medical problems
who are not so ill or unstable that they require evaluation and stabilisation
in ED
• Aim to discharge eligible patients the same day with ongoing clinical
follow-up as required
– Minority that exceed 8pm admitted to MAPU
• Unit comprises chairs (not beds) so patients must be ‘fit to sit’
• Staffed by general physicians and multidisciplinary team with rapid access
to medical diagnostics and procedures
• Patients can be referred from a medical doctor (GP, ED physician, other
specialist), nurse practitioner, or trained paramedic
Ambulatory Emergency Care NHS. Ambulatory Emergency Care – ‘Best Practice’ Case Studies: www.ambulatoryemergencycare.org.uk
Royal College of Physicians. Acute care toolkit 10. Ambulatory Emergency Care. www.ambulatoryemergencycare.org.uk
Directory of Ambulatory Emergency Care for Adults. Version 5, August 2016. NHS Elect 2016
Strang G. The concept, delivery and future of medical ambulatory care. Clin Med 2008; 8: 276-9.
Connolly V, Hamad M. The acute medical take: an outpatient specialty. Clin Med 2008; 8: 21-24.
McCallum L et al National ambulatory emergency care survey:Clin Med 2010;10:555-9.
16. Who’s eligible for AACU?
• List of all emergency medical admissions to PAH between July 1st 2015 and June 30th 2016 with
length of stay <48 hours and which did not involve a stay in SSW.
• 4581 acute medical admissions
– mean (SD) LOS 25.4 (12.6) hours
– 30% of all ~15000 emergency medical admissions
• 2069 (45%) considered potentially eligible for admission to AACU:
– Chest pain – 888 comprising unspecified chest pain (587), other chest pain (212), angina (89)
– Respiratory syndromes – 242 comprising asthma, COPD exacerbation, LRTIs
– Arrhythmias – 221 mostly AF or SVT
– Syncope and collapse – 172
– Congestive cardiac failure – 83
– Dizzy turns – 77
– Orthostatic hypotension – 71
– Minor GI syndromes - 69 comprising GORD, ascites and mild upper GI bleed
– Urinary tract infection – 68
– Transient ischaemic attack – 56
– Cellulitis – 52
– Iron deficiency anaemia – 22
– Anxiety and adjustment disorder – 21
– Transient global amnesia – 17
• Average of 6 patients per day – estimated saving of 4 in-patient beds
17. Impact of AACU
400
400
380
40
Acute Ambulatory
Care Unit (LOS=0 )
MAPU patients
(LOS < 2 days)
1000
400
350
310
50
40
Patients to Inpatient Wards
ED medical attendances
per week
Admitted patients minus
MAPU patients
Admitted patients to
home wards
Admitted patients
1000
Potential for 70 fewer patients/ week moving to in-patient wards
through optimising AACU/MAPU
600 600
Not admitted
Current State Future State
Beware
supply
side
drivers –
AACUs
should
only do
AACU
work
19. Medical assessment and
planning units
• Cohorting patients with defined conditions
• 17 studies of 12 AMUs across five countries
• Reduction in-hospital length of stay (LOS) in all
analyses ranging from 0.3 to 2.6 days
• Reduction in mortality in 12 of the 14 analyses
ranging – up to 8.8%
• Evidence relating to readmissions and patient/staff
satisfaction less conclusive
• Variation admission criteria, entry sources, functions
and consultant work patterns
Reid et al Int J Qual Health Care 2016; Scott et al Int J Qual Health care 2009
20. Focus on older patients
• Early assessment within ED by CGA-trained ED nurses using validated
screening tools to identify and assess older patients who need:
– more support if discharged OR
– rapid transfer to older patient-friendly area for further evaluation and
management
• particular focus on certain patient types: frailty, cognitive impairment,
anxiety/depression, acute delirium or risk of delirium, risk of rapid deconditioning
• emphasis on minimally invasive care and advance care planning
Benefits
• Systematic review confirmed avoidance of hospital admissions and decreased LOS
for those who are admitted (Graf et al 2011)
• Lower admission rates (44% vs 60%), no increased ED revisits (Aldeen et al 2014)
• Reduced admission rates by 12%, and reduced readmissions in people aged 85
years or older discharged from ED by 15% (Conroy et al 2014)
• 33% of older patients presenting to ED discharged same day and LOS for overnight
admitted patients decreased by 18% (Wright et al 2013)
21. Focus on older patients
• Areas within ED or MAPUs that provides older patient-friendly physical
environment and rapid comprehensive geriatric assessment (CGA) and
management
• Physical design and environment more older patient friendly
• Staffed by nurses and AHPs highly skilled in CGA and cognition/delirium management
• Liaison with geriatricians in optimising care and identifying patients who may benefit
from rehabilitation, rapid access to TCP, interim care
• Strong evidence that such areas meet specialised needs of older patients
at risk of delirium, falls and other geriatric syndromes
• Fewer adverse events and reduced mortality
• Less likely to be institutionalised or become more dependent
• Have fewer readmissions to hospital and fewer days in hospital
– Baztan et al 2009; Fox et al 2012; Ekerstad et al 2017
• In the NHS, acute frailty units (AFUs) associated with more rapid exit of at-
risk older patients from ED, with reduction in LOS in ED and improved 4-
hour rule compliance
– Silvester et al 2014; more case studies available at: www.acutefrailtynetwork.org.uk
22. Improving patient flow by
reducing exit block from ED
• Discharge planning from day 0
– Gonçalves-Bradley et al Cochrane Database Syst Rev
2016;(1):CD000313.
• Daily interdisciplinary meetings (huddles)
– Mudge et al Intern Med J 2006;36(9):558-563.
• Daily consultant review
– Bell et al PLoS One 2013; 8(4):e61476
• Expected date of discharge
– Ou et al Aust Health Rev 2011; 35(3): 357-63.
• Flow processes
– Patient flow nurses, nurse navigators
• Review of all long stay patients
– Twice weekly case conferencing
– Prioritised specialty referrals
– Salonga-Reyes, Scott Aust Heath Rev 2017; 41: 54-62.
30. Improving patient flow by removing
delays in acute care
Delays in discharge
when acute care no
longer required
Delays in discharge
when acute care
interrupted by
clinically
inappropriate delays
31. Reducing unplanned
re-presentations to ED
• Discharge nurse co-ordinators and peri-discharge
programs
• Reduce readmissions by up to 20%
» Leppin et al. JAMA Intern Med 2014; 174(7):1095-107; Scott Aust Health Rev 2010; 34: 445-451.
• Prompt discharge summaries
» van Walraven et al. J Gen Intern Med 2002;17(3):186-92.
• Early follow-up and rapid review clinics (<2/52)
» Tung et al. PLoS One 2017;12(1):e0170061
• Chronic disease management
» Scott Intern Med J 2010; 38: 427–437
• Advance care planning
» Scott et al Med J Aust 2013; 199: 662-666; Houben et al J Am Med Dir Assoc 2014; 15: 477–89
• Reduction in inappropriate polypharmacy
» Scott et al JAMA Intern Med 2015; 175: 827-834.
33. Processes within ED
• Rapid streaming and
disposition
• Pull systems and
dynamic floor
management
• Escalation for flow
blockages
33
Improving inpatient flow
• SAFER Flow Bundle
• Overcoming waits
• Interdisciplinary teamwork
Discharge Planning
• Discharge plan from
day 0
• Peri-discharge care
• Stranded patient
policies
Primary care
• Rapid access to consultative
expertise (call lines)
• Rapid access clinics
RACFs
• ED outreach (CARE-PACT)
Mental health
• Rapid response teams
Acute Care
Alternatives to inpatient admission
• Acute ambulatory care unit
• MAPU
• HITH
Inpatient admissions
• Single point referral/acceptance
• Explicit referral criteria
• Rapid admission processes
• Standardised care plans
• Consultant to consultant liaison
• Activation/clinical desk
• Treat and leave
• Ambulance handover
• Avoiding ramping
• Streaming – ‘fast track
ambulatory care’
• Alternative care pathways
Acute Older Patient Care
• Targeting at-risk groups
• Early CGA
• Assertive mobilisation
• Discharge priority
Emergency Care Improvement
Maximising whole of system patient flow
34. Preventative/
predictive care
Chronic disease
management
Alternatives to
admission to
in-patient
wards
Alternative
access for
diagnosis
Alternative
settings for
therapy
Peri-
discharge
care
programs for
reducing
readmission
Health
promotion
General
practice Community
Support
Ambulance
Service ED
SSW
MAPU
AACU
HITH
Focus on CDM and more effective responses to urgent care needs
Clear operational performance framework integrated into primary care
Improved integration with primary care responders
Front load senior decision process
Redesign
to left shift
LOS
Inpatient
wards
Optimise acute
ambulatory care
Information flow converting unheralded ED presentations to heralded presentations
Discharge Process
Maximising whole of system patient flow