Dr. Freeland Article Jan. 2013
•
0 likes•211 views

This article discusses the importance of periodontal health during orthodontic treatment. It notes that poor oral hygiene can lead to decalcification, decay, and gingival infections. The orthodontist should assess the patient's periodontal health and oral hygiene pretreatment. If bleeding or plaque is present, treatment should be delayed until oral hygiene improves. The orthodontist is responsible for ensuring the patient can maintain hygiene during treatment and may need to terminate treatment if hygiene does not improve. Maintaining strong periodontal health leads to on-time case finishes and improved esthetic outcomes and patient satisfaction.

More Related Content
What's hot
What's hot (20)
Similar to Dr. Freeland Article Jan. 2013
Similar to Dr. Freeland Article Jan. 2013 (20)
More from Centric Learning
More from Centric Learning (20)
Dr. Freeland Article Jan. 2013
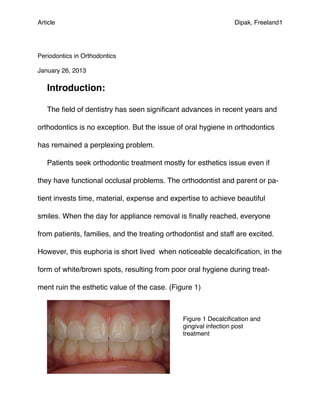
- 1. Article! Dipak, Freeland1 Periodontics in Orthodontics January 26, 2013 Introduction: The field of dentistry has seen significant advances in recent years and orthodontics is no exception. But the issue of oral hygiene in orthodontics has remained a perplexing problem. Patients seek orthodontic treatment mostly for esthetics issue even if they have functional occlusal problems. The orthodontist and parent or pa- tient invests time, material, expense and expertise to achieve beautiful smiles. When the day for appliance removal is finally reached, everyone from patients, families, and the treating orthodontist and staff are excited. However, this euphoria is short lived when noticeable decalcification, in the form of white/brown spots, resulting from poor oral hygiene during treat- ment ruin the esthetic value of the case. (Figure 1) Figure 1 Decalcification and gingival infection post treatment
- 2. Article! Dipak, Freeland2 Patients find it difficult to brush and floss around orthodontic appliances. This leads to a reduction in oral hygiene that results in an increased risk for developing decalcification, decay and gingival infections. The severity of the resultant dental caries can range from development of opaque white- spot lesions (WSL) to the lose of surface integrity of enamel, cavitation and oral caries and periodontal bone loss. As a profession, we need to focus on preventive measures and practices to improve oral hygiene and minimize adverse sequel to the teeth and periodontium. Orthodontists should be aware of the high risk of WSL and decide at the patient level whether it is appropriate to start or continue treatment in pa- tients who are already experiencing enamel demineralization and con- tinueal gingival inflammation. The risk of developing incipient caries and gingival lesions during orthodontic treatment should not be underestimated by orthodontists. Research indicates that 49.6% of orthodontic patients exhibit enamel opacities on at least one tooth after orthodontic treatment. There is a sig- nificant risk that 1 in every 10 bonded teeth is likely to have post-treatment white spots with the incidence in banded teeth being slightly more at 1 in 9
- 3. Article! Dipak, Freeland3 teeth. A significant increase in incidence, prevalence and severity of enamel opacities following orthodontic treatment has also been reported in the same study. 1 A number of factors are responsible and the authors have attempted to highlight a few and discuss them. Factor One: Pretreatment patient assessment At the initial exam the doctor should perform a complete periodontal exam that assess the health of the periodontium and the patients oral hy- giene. If the oral exam shows plaque accumulation and gingival bleeding then this patient should not be considered for orthodontic treatment until the gingival tissues are completely healthy. Figure 2 Figure 2: An example of poor oral hygiene pretreatment. This type of patient should not be treated until the gingi- val problems are rectified.
- 4. Article! Dipak, Freeland4 Factor Two: How to identify oral hygiene problem patients With the tooth brush the doctor places the bristles into the sulcus area in the anterior and posterior areas. If bleeding occurs then there is a hygiene problem. (Figure 3) Figure 3: A toothbrush is used in place of a periodontal probe. This way the parent/patient can not ac- cuse the practitioner of cutting the gums. Factor Three: How to improve patients oral hygiene. At this time a preventive dental program should be introduced. If the pa- tient still shows gingival bleeding after the program then he/she should not be placed in orthodontic treatment. This program should be designed to
- 5. Article! Dipak, Freeland5 enhance the diagnosis so the Doctor and patient can discover the oral hy- giene problems together. The preventive program has five parts. The first two appointments are 1 week apart and the proper techniques for oral hygiene are taught and re- viewed. The next three appointments should show complete gingival health over a 3 months period. If this is not the case then orthodontic treatment should be withheld from this individual. It is the responsibility of the ortho- dontist to withhold treatment because if the patient will not take of the teeth and gums before treatment there oral hygiene will not improve during treatment. 2 A close relationship with the referring dentist and his hygiene staff will facilitate the efforts of the orthodontist. Making sure the patient sees the dentist/hygienist more often may help reinforce the orthodontist efforts to obtain a disease free mouth.
- 6. Article! Dipak, Freeland6 Factor four: Oral hygiene problems during appliance therapy (Fig 5) Figure 5: The appliance system does increase the oral hygiene problems. Once treatment begins the orthodontist is responsible for proper instruc- tion on how to managed the hygiene issues created by the appliances. The proper use of the brush and floss should be demonstrated by the doc- tor. If the doctor spends the time it will impresses on the parent/patient the importance of oral hygiene. 3 (Figure 6,7) Figure 6: Flossing should be demonstrated. Espe- cially how the patient gets the floss into the sulcus.
- 7. Article! Dipak, Freeland7 Figure 7: Brushing needs to be taught. The demonstration should include how to get the bristles into the sulcus. The doctor should create an appliance environment that enhances the patients ability to care for the gingiva and enamel. All flash from bonding and banding should be removed. The use of sealants, such as Proseal, as part of the bonding procedure should be instituted. The bonding system should contain fluoride. The use of mechanics systems and retention sys- tems that make it difficult to clean should be avoided. In the light of the pa- tients past oral hygiene issues during appliance therapy, bonded retainers, should be avoided. As bonded retainers are placed “invisibly on the lingual tooth surfaces, patients’ acceptance is evident. This practice may lead to the development of carious lesions, favor the formation of plaque and cal- culus around the mandibular retainers, compared to the maxilla.7
- 8. Article! Dipak, Freeland8 Zacchrisson, 4 one of the pioneers in the field of bonded lingual retain- ers, stressed the importance of daily interproximal cleaning with dental floss. Despite optimal oral hygiene instructions, calculus formed to a greater extent on the lingual surfaces of the incisors with bonded retainers, compared with incisors without bonded retainers. 7 The patient is responsible for the care of the teeth and gingival tissues. if all efforts have failed and the oral hygiene does not improve then the or- thodontist should consider terminating treatment. Even if it is unilateral de- cision on the orthodontist part: Jerrold 6 explains that the doctor-patient relationship is bilateral and consensually based. He further elaborates that once in existence, this rela- tionship can be dissolved in 5 ways: (1) both parties agree to end it (a common example is when the patient is relocating: (2) The patient’s condi- tion is cured, and no further treatment is required: (3) the doctor or patient dies: (4) the patient decides to unilaterally terminate the relationship; or (5), the doctor decides to unilaterally terminate the relationship. Jerrold further elaborates by suggesting that the doctor can unilaterally terminate the relationship if the patient breaches at least 1 of the 5 duties owed to the practitioner under the contract that comprises the doctor-
- 9. Article! Dipak, Freeland9 patient relationship: (1) the patient is not following the doctor’s instructions regarding treatment and thus is jeopardizing his own treatment; (2) the pa- tient is not keeping appointments, thus causing interruptions in the continu- ity of care, not to mention the interference with the business aspect of the doctor’s practice: (3) the patient is not being truthful or forthcoming regard- ing necessary administrative inquires(e.g. his medical history, information about those financially responsible for his care, his degree of cooperation, signs and symptoms of problems, and so on); (4) the patient is not con- forming to accepted modes of behavior (he is belligerent or abusive to the doctor or his staff,m or is crating a hostile or unhealthy environment in the office; and (5) the patient is not paying for services rendered. 6 (Figure 8) Figure 8: A case where the patient would not follow oral hygiene program so treatment was dis- continued. In all fairness to the patient, some patients will exhibit gingival swelling in response to the appliances during treatment. It begins within a couple of
- 10. Article! Dipak, Freeland10 months after placement of the appliances. Fixed appliances predispose plaque accumulation and colonization of bacteria. When gingival tissues are enlarged, the tooth surfaces/bracket tooth interface become difficult to access, inhibiting good oral hygiene and resulting in an increase in inflam- mation and bleeding. The interruption of orthodontic treatment is often ad- vised when gingival enlargement is diagnosed. The temporary removal of the irritating factors such as attachments and appliances, debridement, chlorhexidine prophylaxis, and in some patients, surgical intervention as as flap/laser surgery, to restore the contour of the enlarged gingival tissues, can facilitate adequate oral hygiene during subsequent orthodontic treat- ment. 4 Conclusion: The benefits to the practice are enhanced in many ways by having all patients gingiva disease free while under the orthodontic care. Increased patient referrals will occur because their cases are finished on time with a beautiful smile that is enhanced by healthy gingival tissues and teeth free of decalcification. 5 Increased referrals from the dental profession will occur when their patients are being well taken care of while in the orthodontist
- 11. Article! Dipak, Freeland11 practice. A study on marketing forces failed to discern or ascertain the degree/depth of the emotional connection created between the orthodontist and patient. 5 This doctor patient relationship is the most important aspect in finishing cases with healthy gingival tissues and free of decalcification. The patient/parent will differentiate services offered by different prac- tices. They will choose the practice that develops the bonds necessary to create the healthy oral environment. This will enhance the patient satisfac- tion at the end of treatment. Even if the cases are walk-in/google/patients referral cases, because we will be judged by the general dentists at the oral hygiene appointments. Other benefits to the practice are on time finishes. A healthy oral envi- ronment always finish on time. The esthetic value is always present so at post treatment consultations the parents/patients are most willing to refer their friends to your practice. The time spent trying to improve oral health is one of the best practice building technique. Better then all the marketing techniques combined. (Figure 9)
- 12. Article! Dipak, Freeland12 Figure 9: Completed case where the patient followed the oral hygiene pro- tocol. Not only did she finish ahead of time she finished with a great smile. References: 1. Gorelick 2. Barkley RF. Successful Preventive Dental Practice Amazon 3. Yeung 4. Zachrison 5. Beckwith 6. Jerrold 7. Orsborn Authors: Dr Dipak Dr Ted Freeland DDS, MS Past adjunct professor University of De- troit orthodontic department. Twice Board certified, Director Advanced Education in Orthodontics. Private Practice.
- 13. Research Paper! Last Name 13