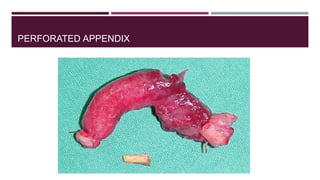
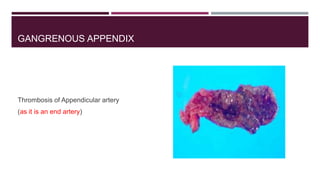
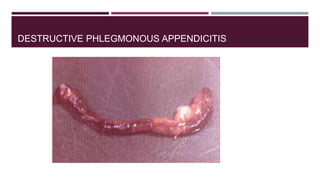
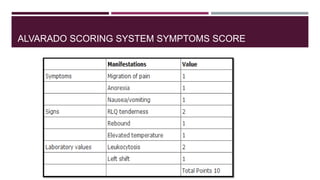
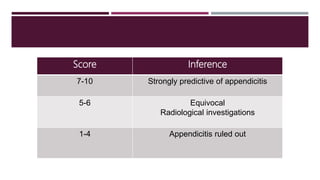
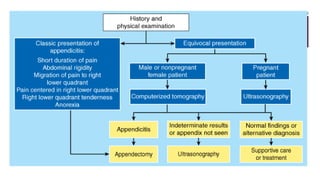
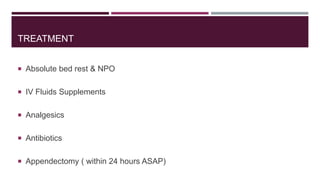
This document discusses acute appendicitis, its complications, and treatment options. It notes that appendicitis is caused by obstruction of the appendix lumen, leading to congestion and increased pressure. Left untreated, it can progress to gangrenous appendicitis or perforation. Complications include peri-appendiceal abscess, peritonitis, and sepsis. Diagnosis involves symptoms, signs, and tests like bloodwork and imaging. Treatment is usually appendectomy within 24 hours, while conservative treatment with antibiotics may be used for appendicular lumps in some cases.