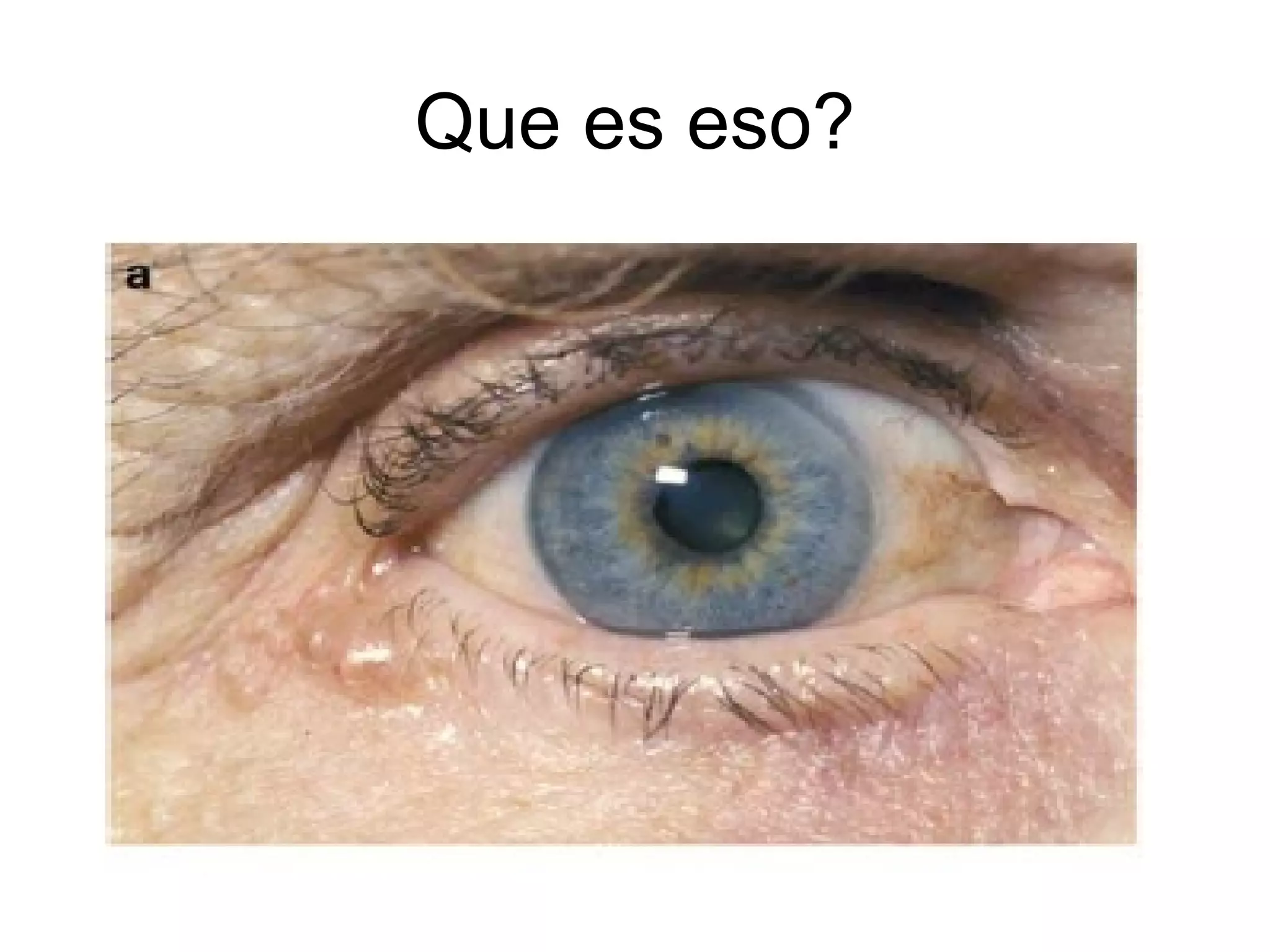
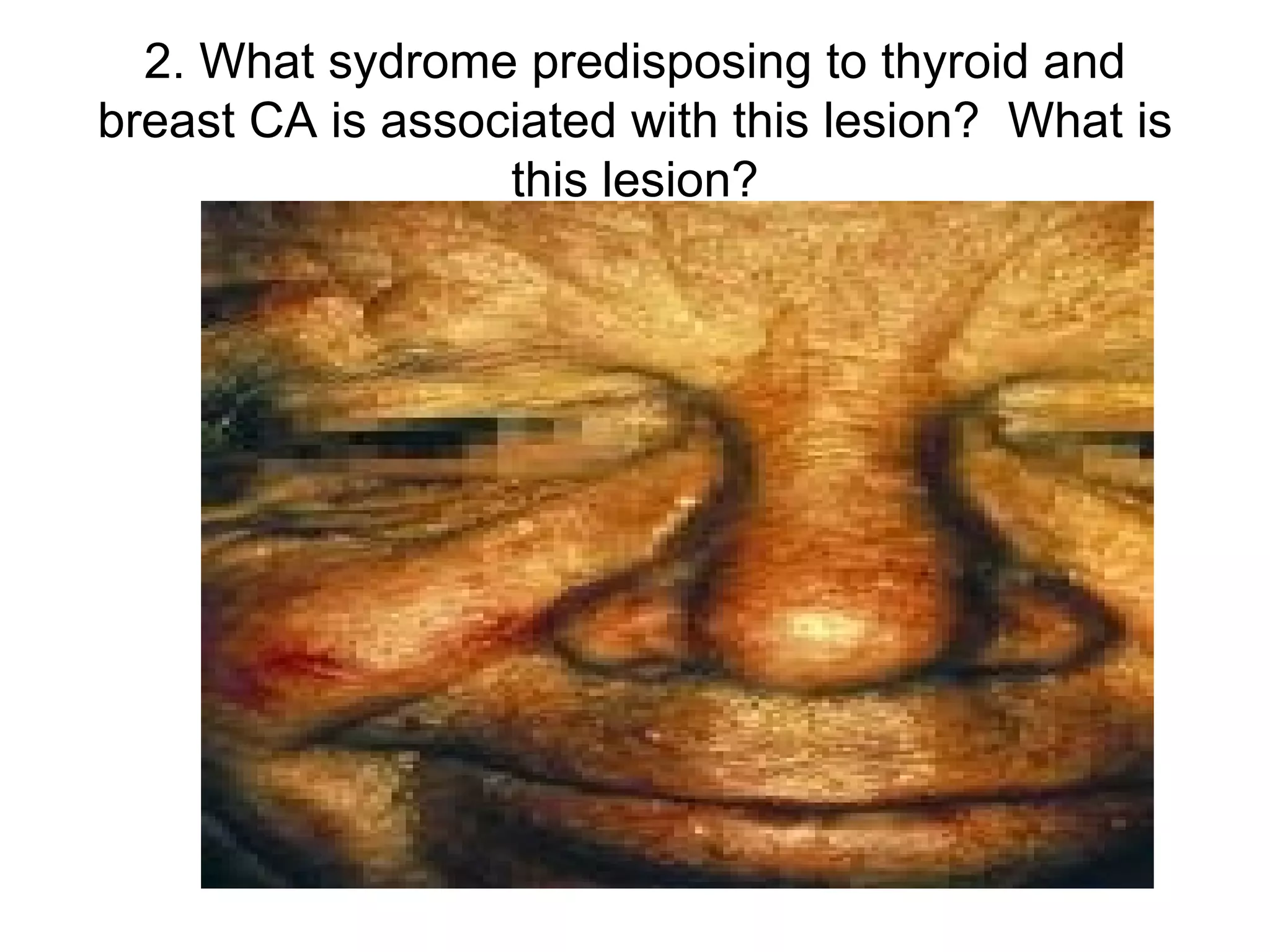
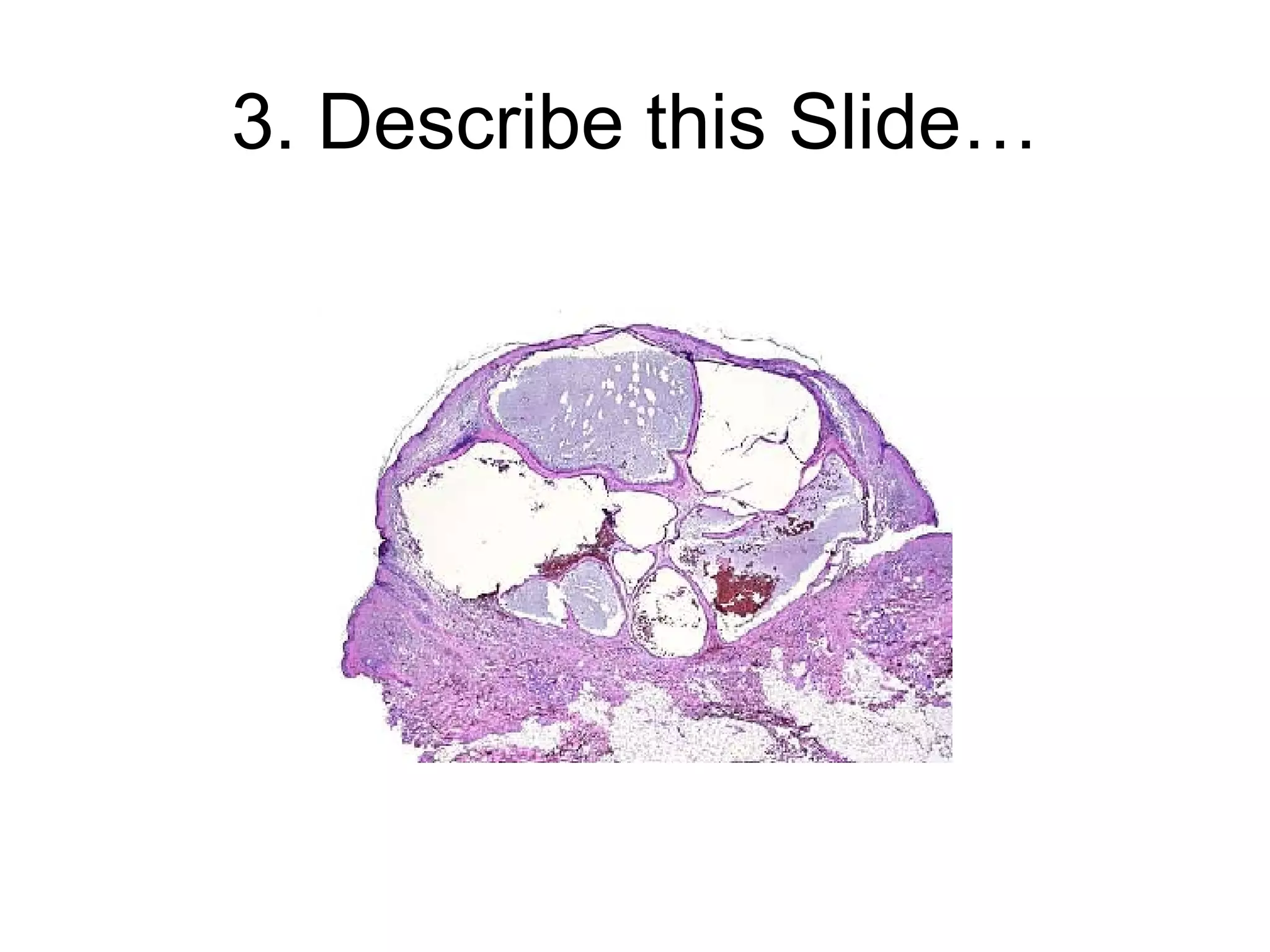
The document describes a case presentation of a 55-year-old male with a lesion on his left eye that was diagnosed as an apocrine hidrocystoma. Apocrine hidrocystomas are benign cystic proliferations of the apocrine glands that commonly appear as solitary, soft, dome-shaped papules or nodules on the eyelids. Histological examination showed multiple cystic areas lined by apocrine-type secretory epithelium, confirming the diagnosis. Treatment options include incision, drainage, electrosurgical destruction or excision to prevent recurrence.