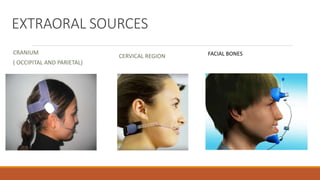
This document discusses anchorage, which refers to resistance to unwanted tooth movement during orthodontic treatment. It defines anchorage and classifies it according to source, jaws involved, site, number of units, and amount of contribution to space closure. Intraoral sources include teeth and alveolar bone. Extraoral sources are the cranium, facial bones, and neck. Anchorage can be simple, stationary, or reciprocal. Methods to maximize anchorage and minimize loss are also described, such as headgear, implants, and anchorage planning.





















































![lecture_05_and_06-Anchorage_in_orthodontics[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture05and06-anchorageinorthodontics1-240224004209-047377b5-thumbnail.jpg?width=640&height=640&fit=bounds)



























