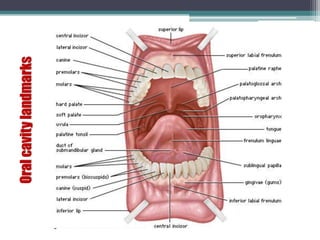
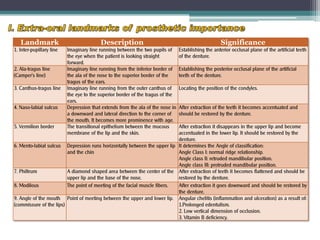
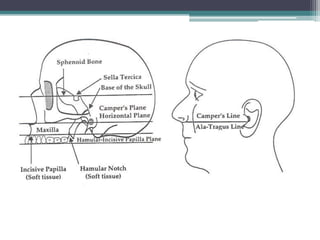
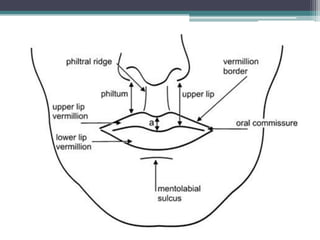
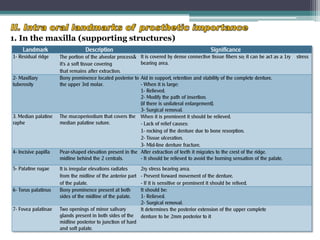
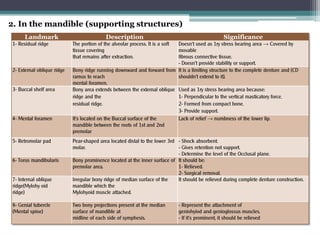
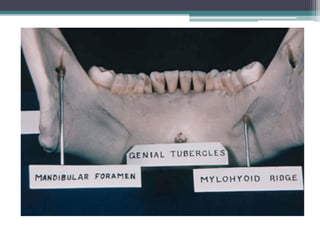
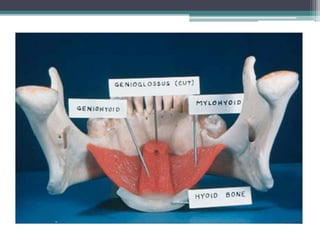
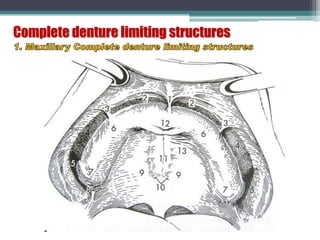
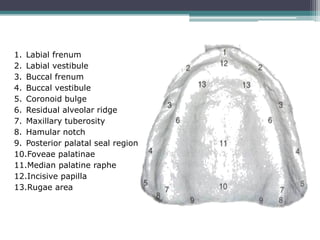
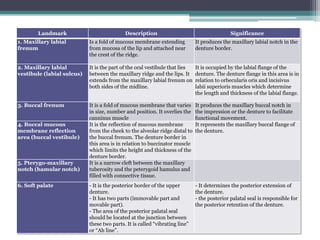
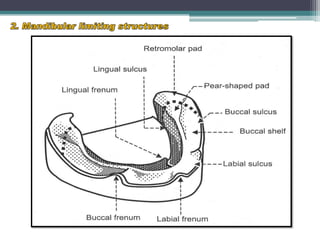
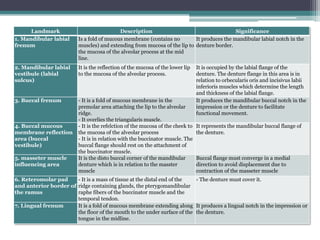
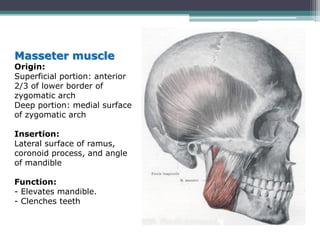
This document discusses important oral anatomy landmarks that are relevant to denture construction. It describes both extra-oral and intra-oral landmarks in the maxilla and mandible, including frenums, vestibules, ridges, tuberosities and other structures. The landmarks are described in terms of their location, appearance and significance for guiding denture border design. Key muscles like the masseter, temporalis and pterygoid muscles that influence denture retention and stability are also outlined. Understanding these oral landmarks and muscles helps the operator properly construct removable dentures.






























![Recent advancements in denture base materials [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancementsindenturebasematerialsautosaved-181219143003-thumbnail.jpg?width=640&height=640&fit=bounds)





![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)


































