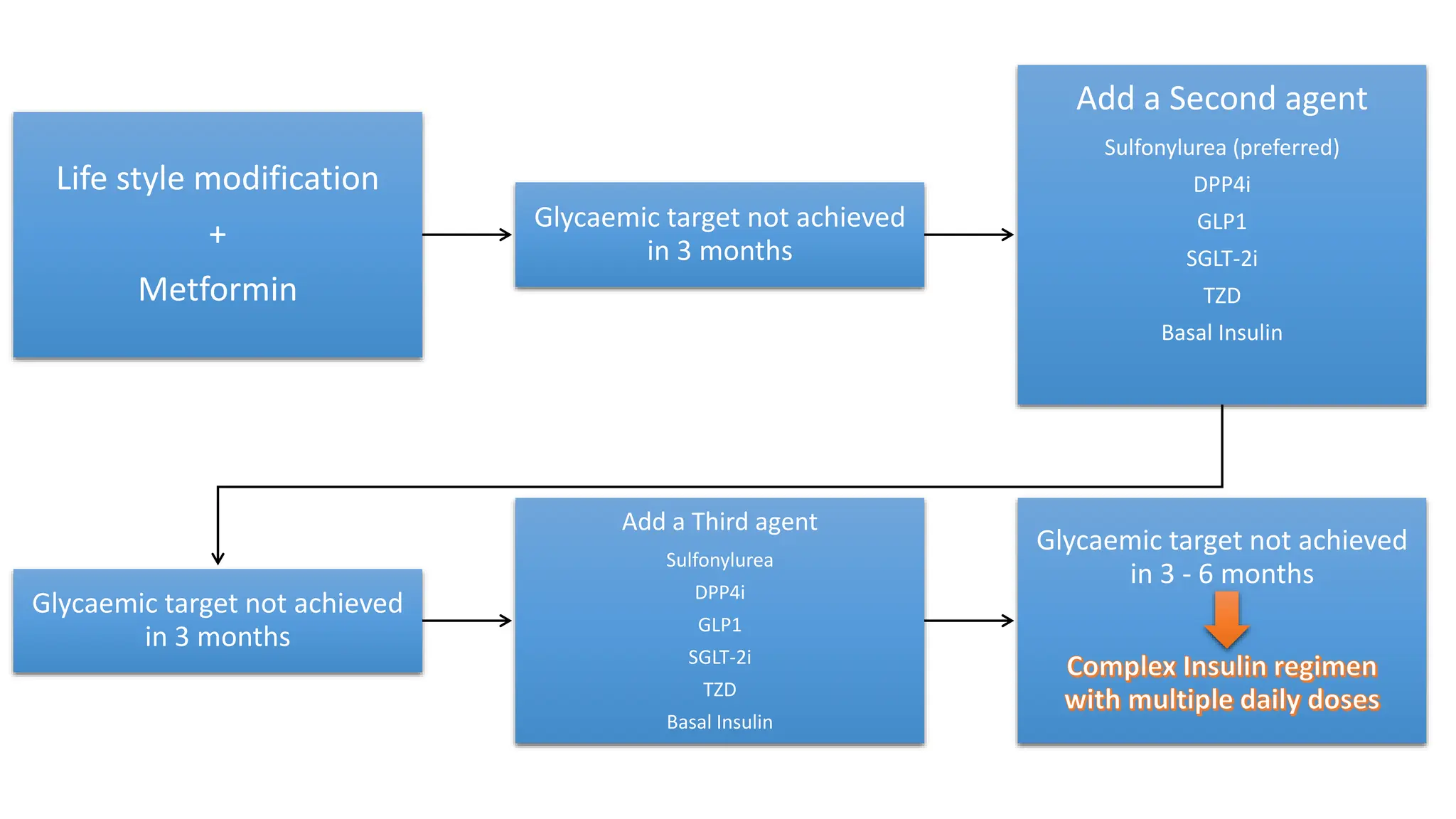
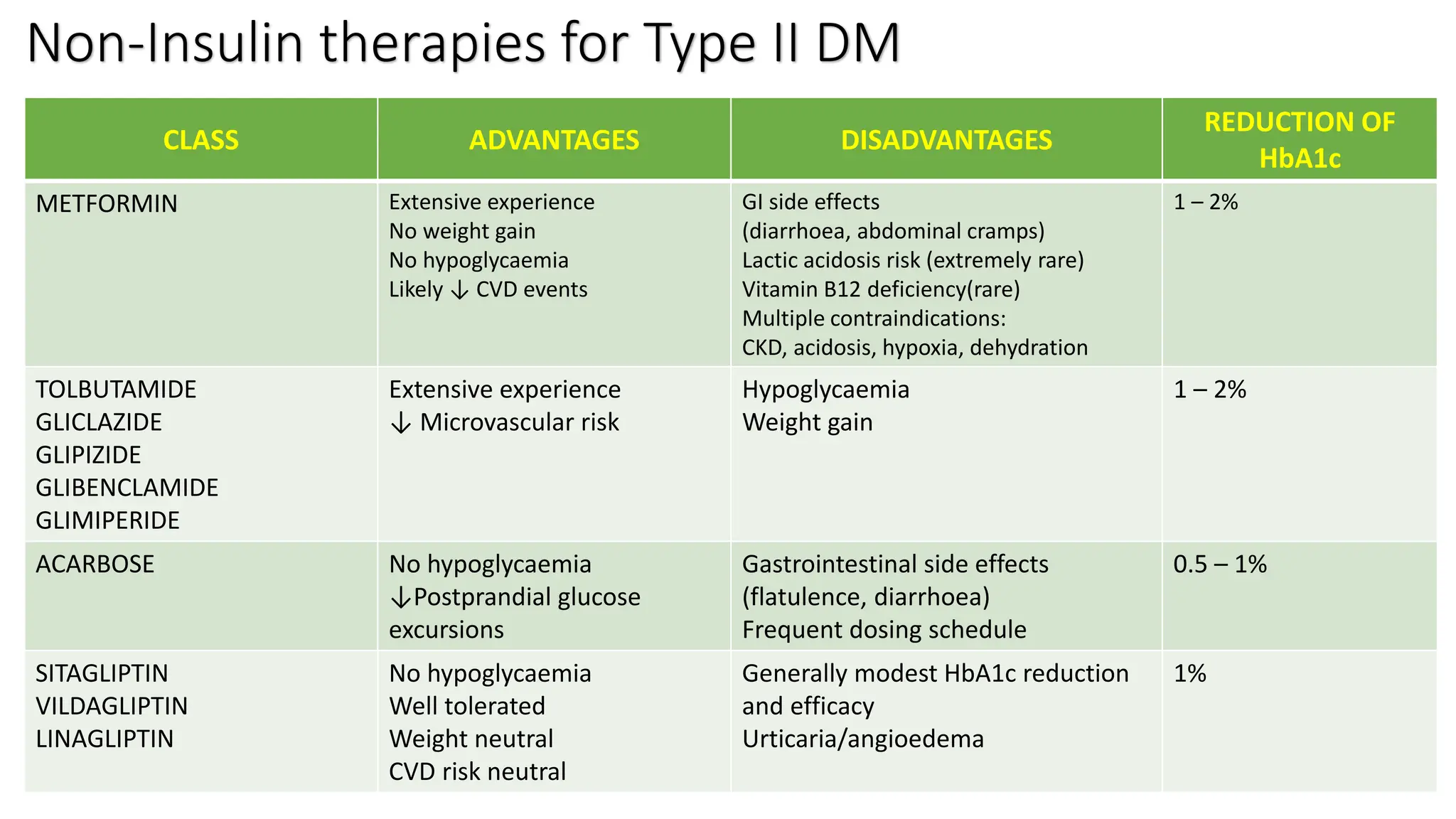
This document provides an update on diabetes mellitus, including its classification into four main subtypes, diagnostic criteria, screening recommendations, treatment goals, and management strategies. Type I diabetes is characterized by absolute insulin deficiency due to autoimmune destruction of beta cells. Type II diabetes accounts for 90-95% of cases and involves relative insulin deficiency and insulin resistance. Diagnosis is based on fasting plasma glucose, oral glucose tolerance testing, or HbA1c levels. The main goals of management are lifestyle modification, glycemic control, risk factor reduction, and prevention of complications through medical nutrition therapy, physical activity, pharmacotherapy including metformin and additional agents as needed.