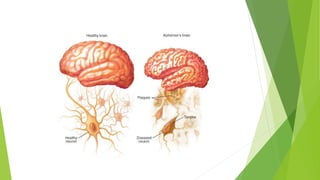
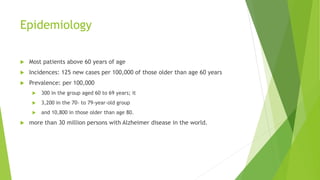
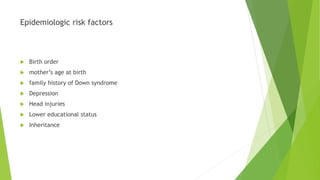
Alzheimer's disease is the most common cause of dementia. It was first described in 1907 when a woman exhibited a progressive dementia over 5 years. It mostly affects those over age 60, with rates of affected individuals rising significantly with age. Risk factors include family history, depression, and lower education. Clinically it presents with amnesia, language problems, and cognitive decline. Diagnosis involves clinical evaluation and tests of cognition along with ruling out other conditions. Pathology shows brain atrophy and plaques and tangles in brain tissue. Current treatments can provide mild cognitive benefits but do not stop progression of the disease.






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












