Downloaded 55 times



































































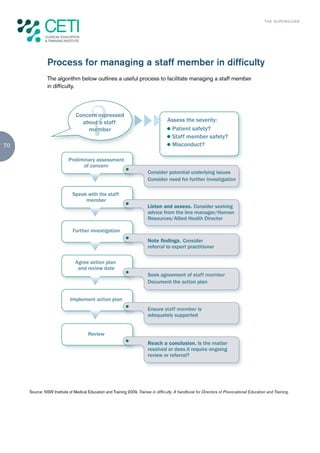

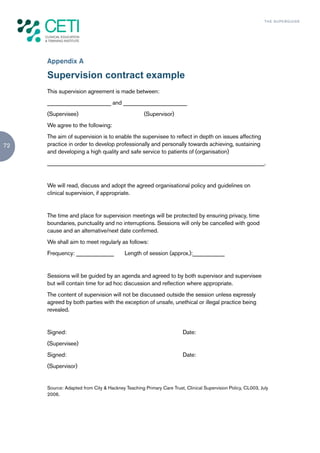
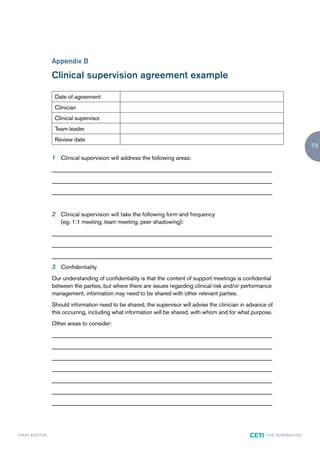

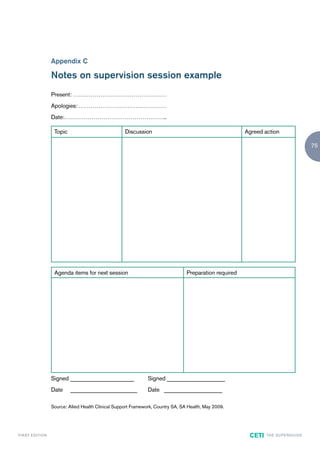


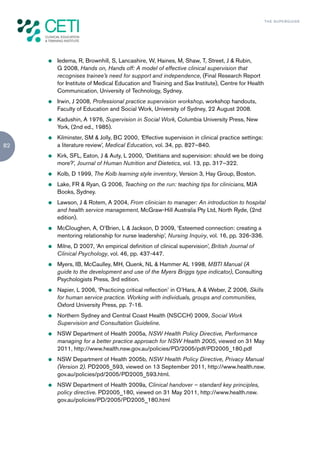






This document provides guidance for supervising allied health professionals. It discusses the purpose of clinical supervision which is to facilitate high quality patient care, learning and professional development, accountable decision making, and staff well-being. Effective supervision involves setting clear expectations, promoting lifelong learning, and ensuring supervisees are active participants. Supervisors should understand adult learning principles and styles to effectively contribute to professional development. Maintaining patient safety is the top priority for both supervisors and supervisees.

























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





