Download to read offline

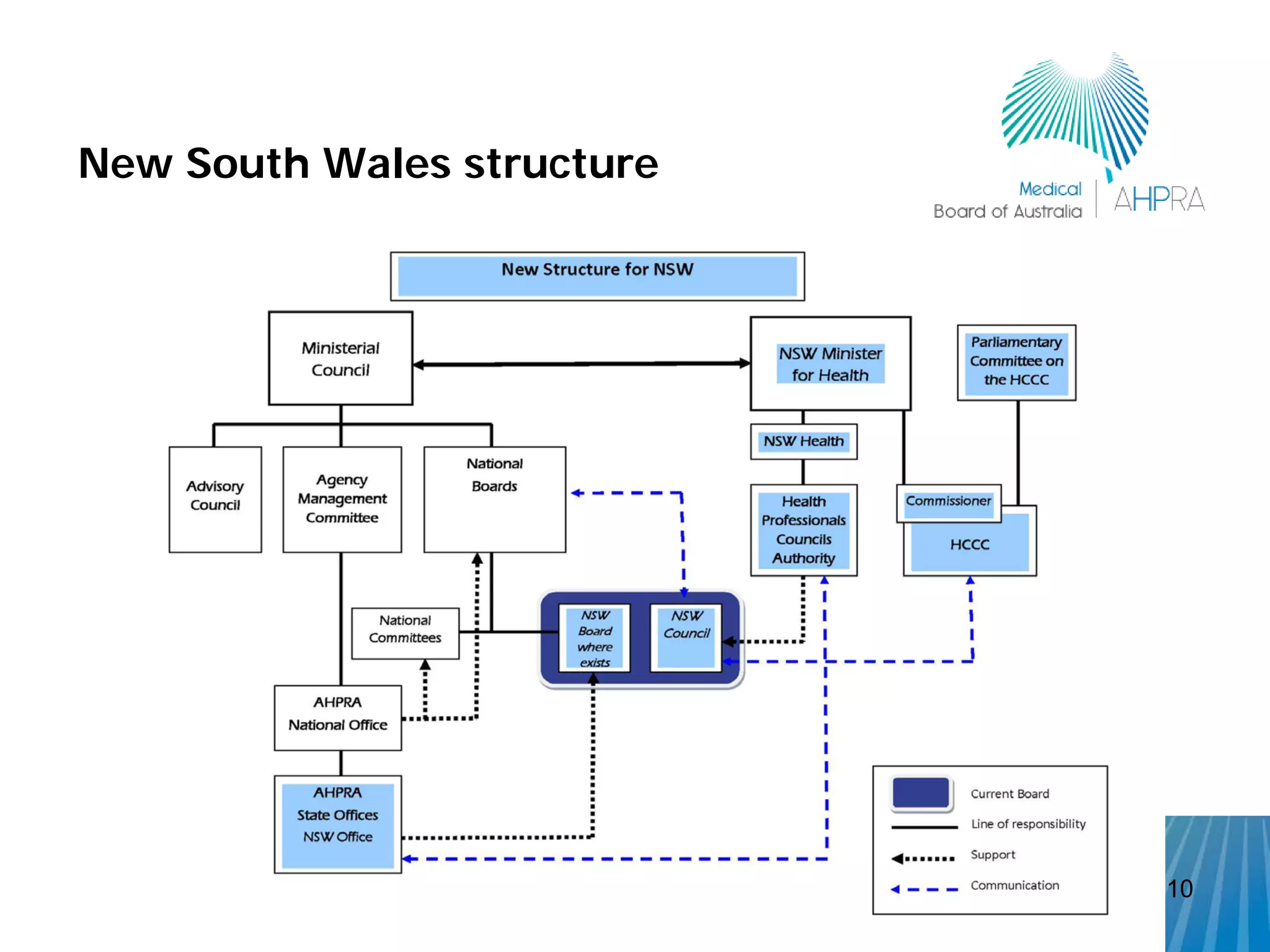



The document outlines the establishment of a national registration and accreditation scheme for health professionals in Australia, effective from July 1, 2010. It details the framework and responsibilities of various boards, including the Medical Board of Australia, regarding the registration standards and accreditation of interns. Key features of the intern year and performance assessments are also discussed, highlighting changes in policy, consistency across jurisdictions, and mandatory reporting obligations for registered practitioners.



































































