This document discusses alcohol related brain damage (ARBD), a spectrum of neurological and cognitive conditions caused by chronic alcoholism. It describes several specific conditions under the ARBD umbrella, including Wernicke's encephalopathy and Korsakoff's syndrome. Wernicke's encephalopathy is an acute neurological disorder caused by thiamine deficiency, with symptoms including eye movement abnormalities, gait issues, and altered consciousness. Korsakoff's syndrome is a chronic memory disorder that can develop after Wernicke's encephalopathy, characterized by anterograde amnesia and confabulation. The document outlines the molecular mechanisms, neuroimaging features, and neural substrates of these conditions.




![WERNICKE’S ENCEPHALOPATHY
• Acute neurologic disorder secondary to nutritional Thiamine
deficiency ; Mortality 20%; WE KS (80%)
• Triad [10%]: Opthalmoplgeia , Ataxia, Disturbances of
consciousness
• Opthalmoparesis [30%]: (Bilateral; Asymmetrical) Horizontal
nystagmus, LR palsy, Gaze palsy, Ptosis, INO; Pupils:
Anisocoria, sluggish reaction to light
• Ataxia: LL; gait disturbances
• Alterations in level of consciousness: acute confusional state;
inattention, disorientation, drowsiness, stupor, pre-coma, coma
• Hypotension, hypothermia, tachycardia: Hypothalamic
involvement
• Axonal Polyneuropathy
• Gratifying and prompt response to Thiamine](https://image.slidesharecdn.com/alcoholrelatedbraindamage-230818075415-ea368a99/75/Alcohol-Related-Brain-Damage-ppt-8-2048.jpg)



















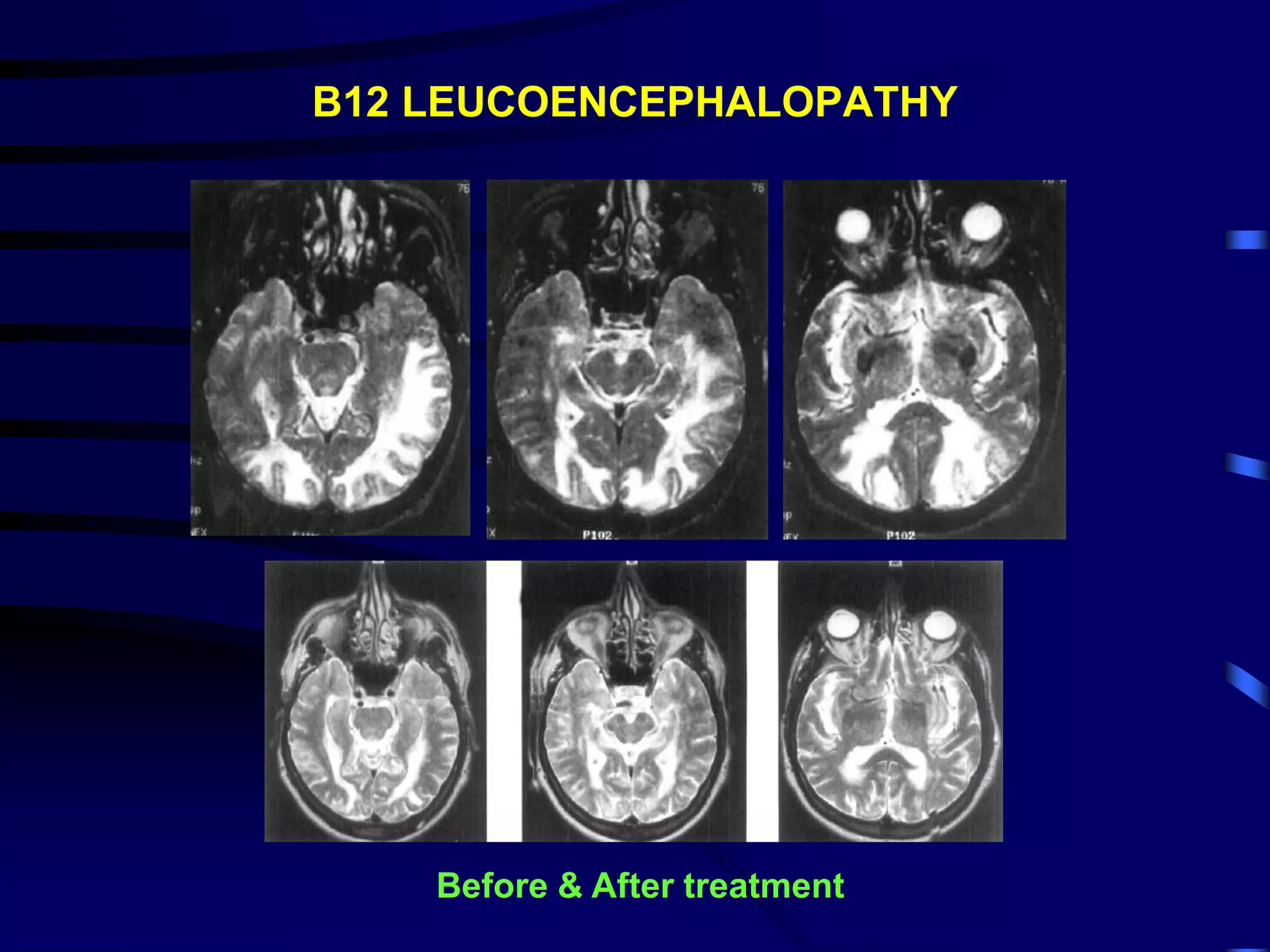
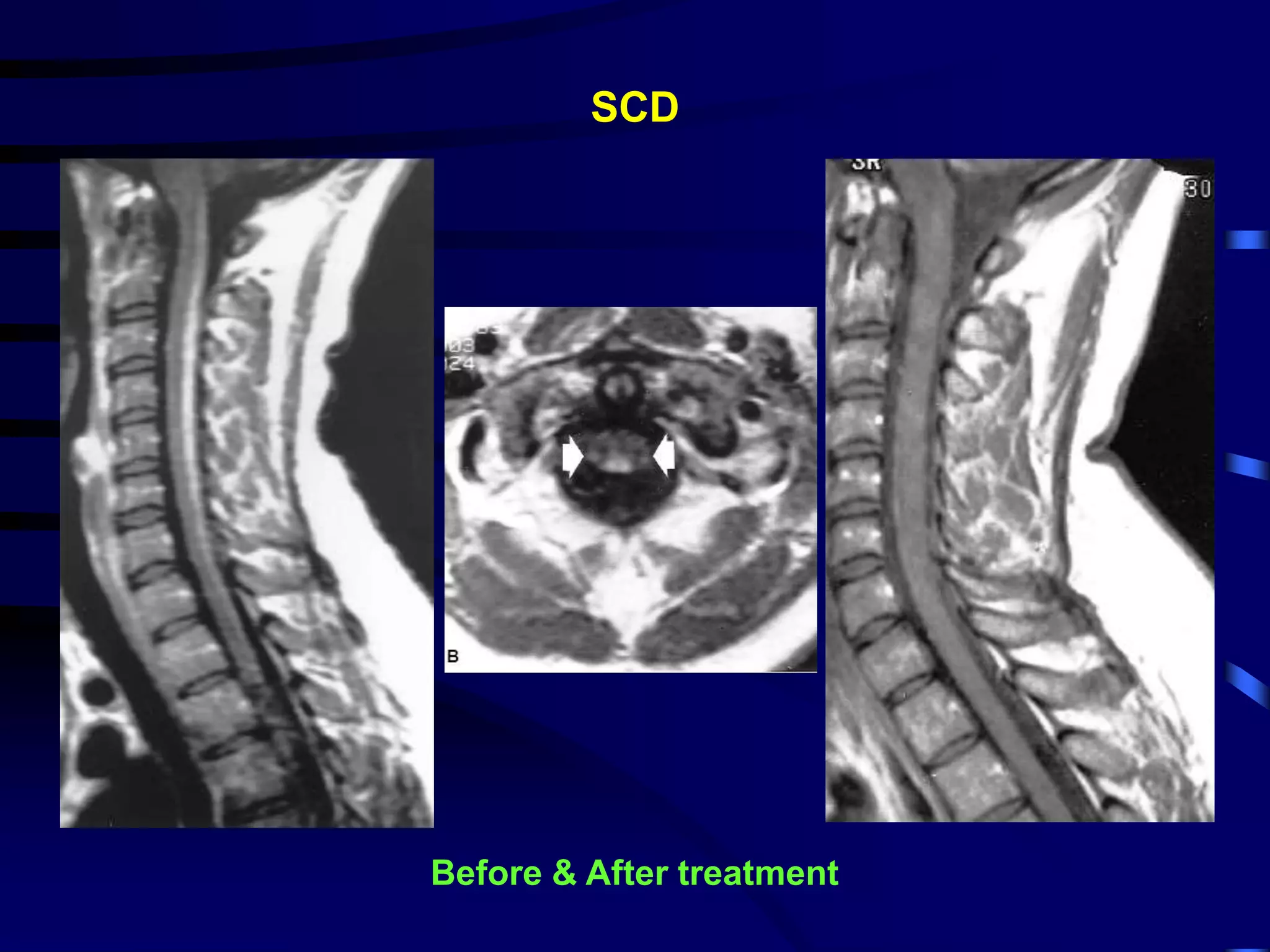
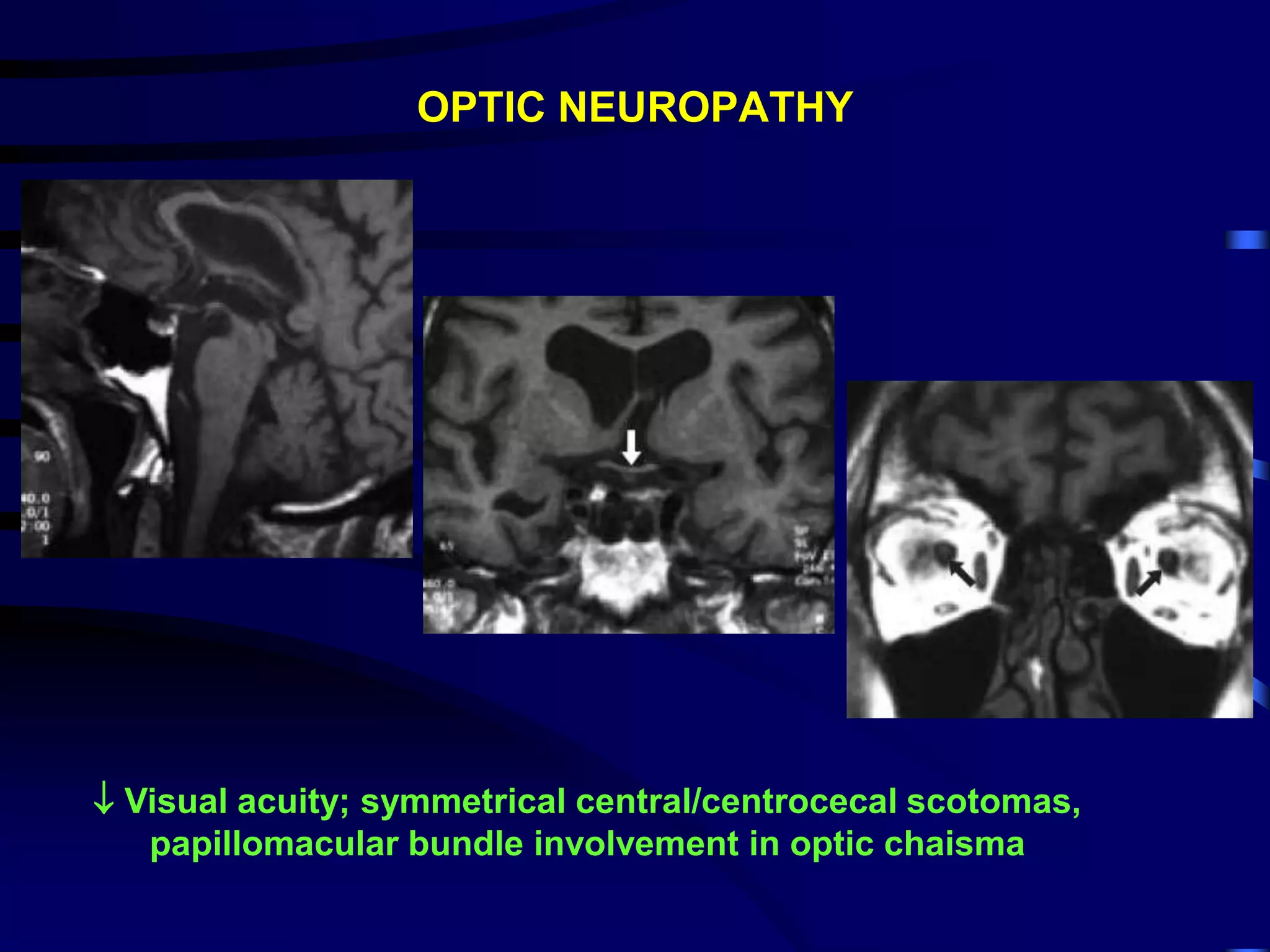
![VITAMIN B12 RELATED NEUROLOGIC DISORDER
• Dementia
• Neuropsychiatric symptoms: personality changes, depression,
affective syndromes, psychosis (“megaloblastic madness”),
delusions, hallucinations, mania, ataxia
• Optic neuropathy, peripheral neuropathy, SCD
• Symptoms occur commonly in the absence of anemia, or
elevated MCV, a borderline low serum cobalamin: not rare and
should not be considered as evidence against the diagnosis of
cobalamin deficiency
• Useful confirmatory evidence of cobalamin deficiency: elevated
serum levels of methylmalonic acid (MMA) and total
homocysteine (Hcy) [100% specificity] ; with treatment MMA &
Hcy levels normalises (Lindenbaum J. NEJM 1988; 318:1720-
1728)](https://image.slidesharecdn.com/alcoholrelatedbraindamage-230818075415-ea368a99/75/Alcohol-Related-Brain-Damage-ppt-46-2048.jpg)