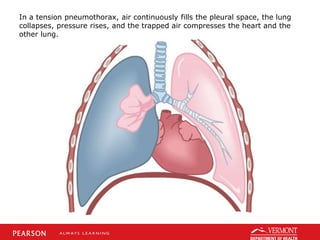
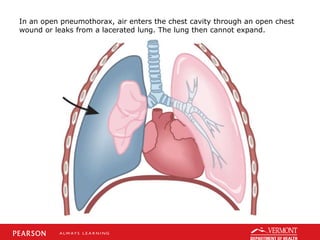
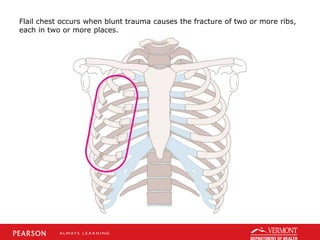
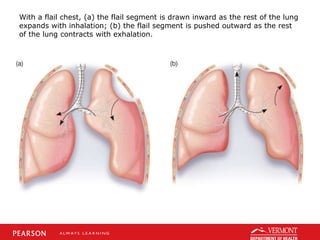
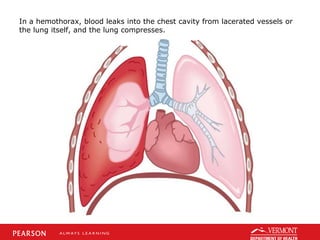
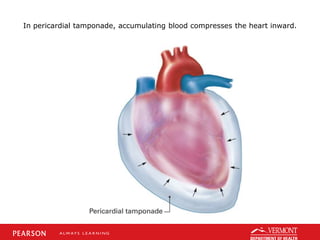
This document discusses chest trauma, including epidemiology, pathophysiology, assessment findings, differential diagnosis, and emergency medical care. It provides case studies to illustrate key points. Regarding pathophysiology, it describes how conditions like tension pneumothorax, open pneumothorax, flail chest, and hemothorax can occur from chest trauma and affect ventilation and circulation. Emergency medical care focuses on maintaining the airway, breathing, and circulation while providing full immobilization and rapid transport. Case studies demonstrate assessing and managing a potential chest trauma patient.