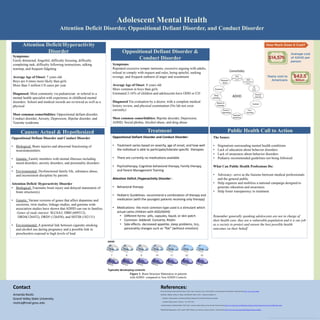
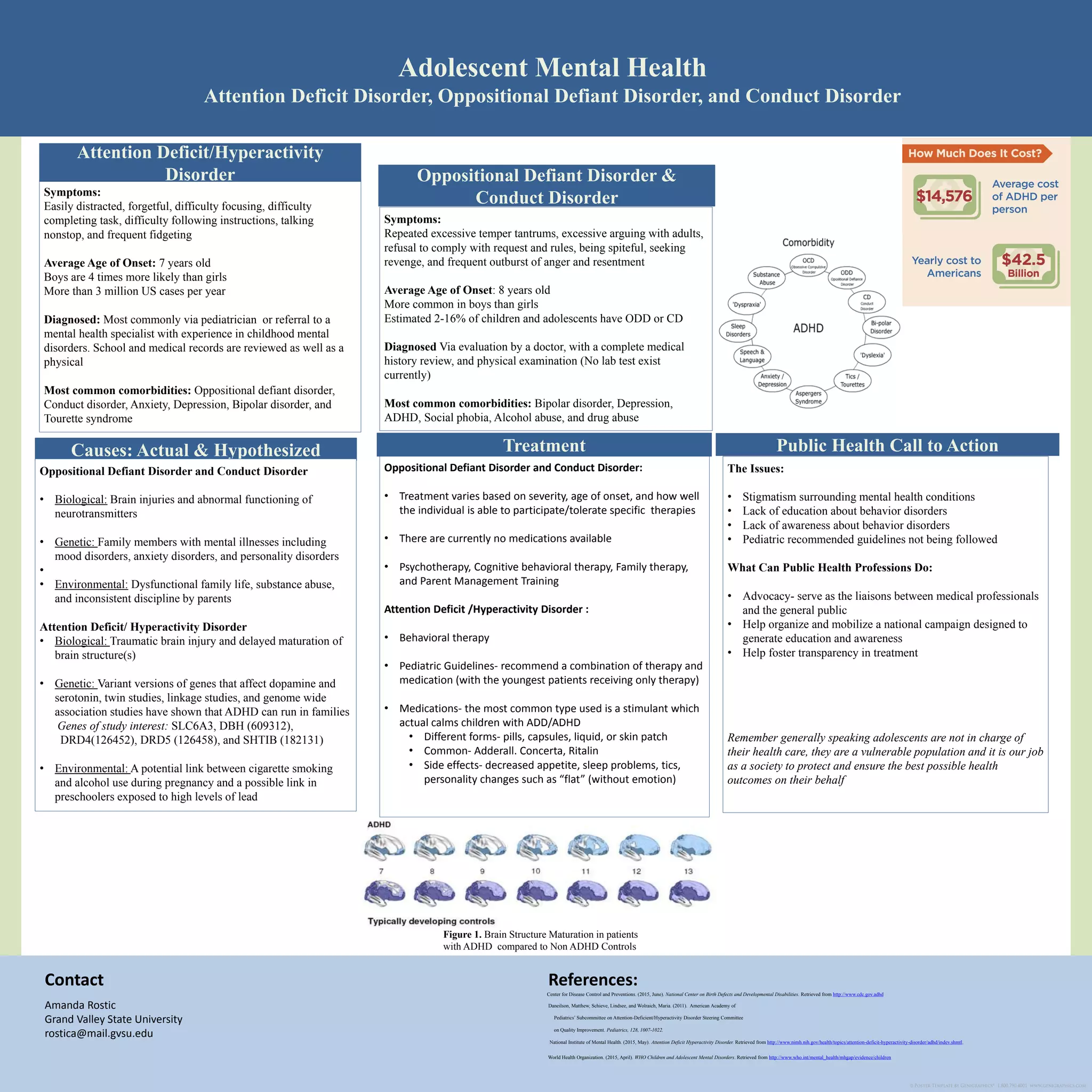
The document discusses common childhood mental disorders, specifically attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), and conduct disorder (CD), outlining symptoms, average ages of onset, and treatment options. It emphasizes the need for public health advocacy to raise awareness and education about these disorders, and addresses misconceptions and stigmas surrounding them. Additionally, it highlights biological, genetic, and environmental factors contributing to these disorders.