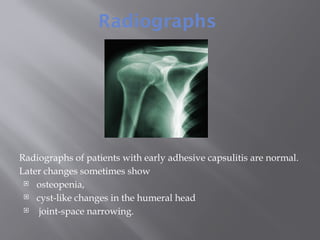
Adhesive capsulitis, or frozen shoulder, is a painful condition characterized by severe stiffness and limited mobility in the shoulder, affecting daily activities. The condition progresses through three stages: freezing, frozen, and thawing, with recovery often being incomplete. Risk factors include diabetes and age, and while radiographs may show normal findings initially, diagnostic tests should differentiate it from other shoulder issues.