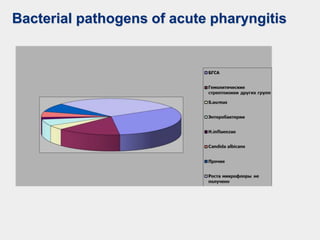
The document discusses acute pharyngeal diseases, focusing on causes, symptoms, and treatment options for conditions such as acute pharyngitis and acute tonsillitis. It highlights the role of various infectious agents, including viruses and bacteria, in these diseases and outlines clinical symptoms and necessary diagnostic methods. Treatment strategies involve dietary recommendations, topical remedies, and the careful use of antibiotics, with a generally favorable prognosis for most cases.









































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




