This document discusses acute appendicitis, including:
1. The pathophysiology of appendicitis is obstruction of the appendix lumen by fecoliths, lymphoid hyperplasia, or other causes, leading to inflammation, edema, and impaired blood flow.
2. Physical exam findings include migrating pain from the umbilicus to the lower right abdomen, tenderness over the right lower quadrant, nausea, vomiting, and fever.
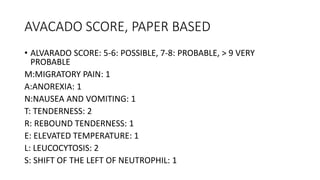
3. Investigations show leukocytosis, elevated CRP, and imaging findings on ultrasound, CT, or X-ray of an enlarged appendix. The Alvarado score is used to assess likelihood of appendicitis.
4.