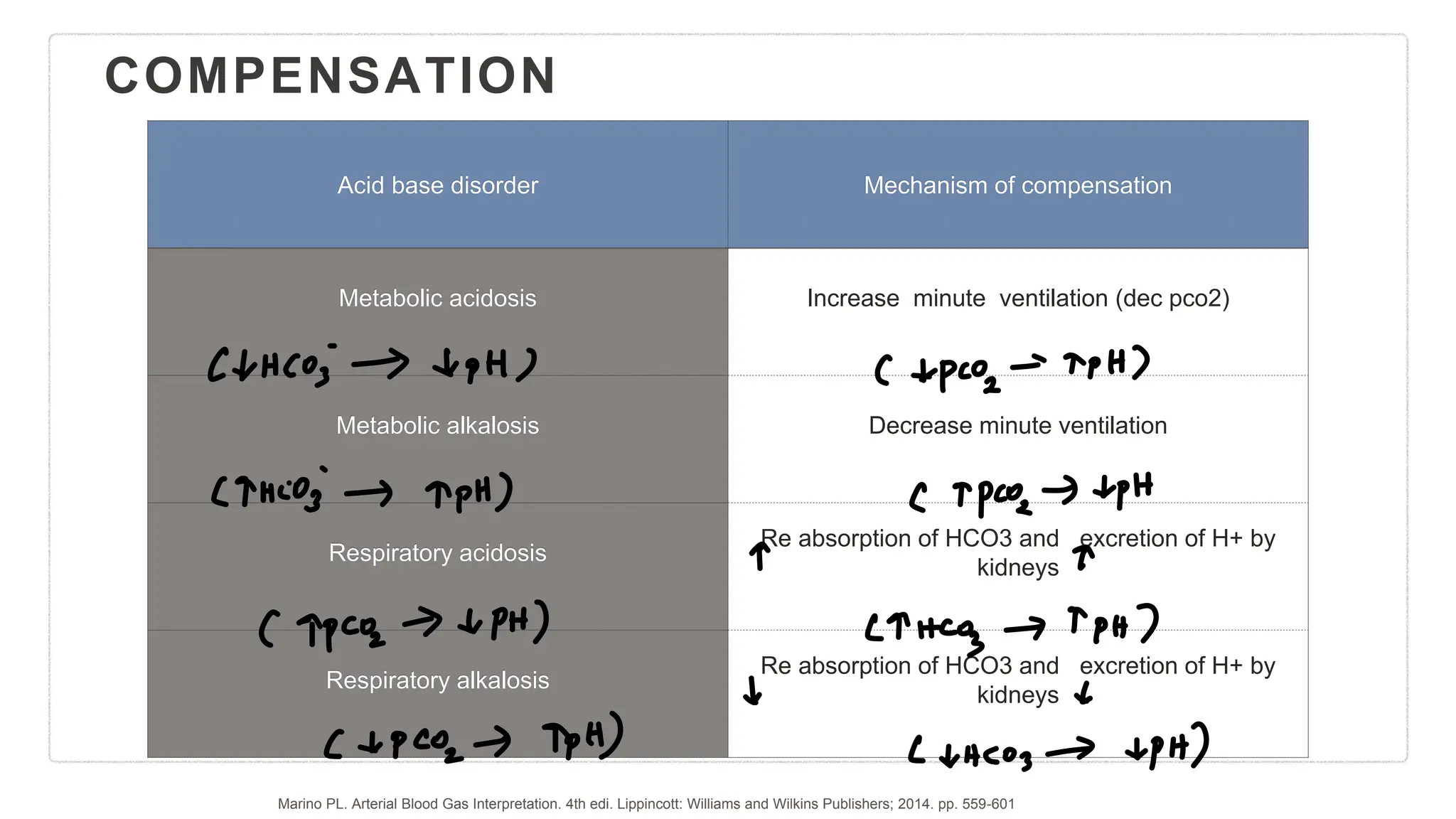
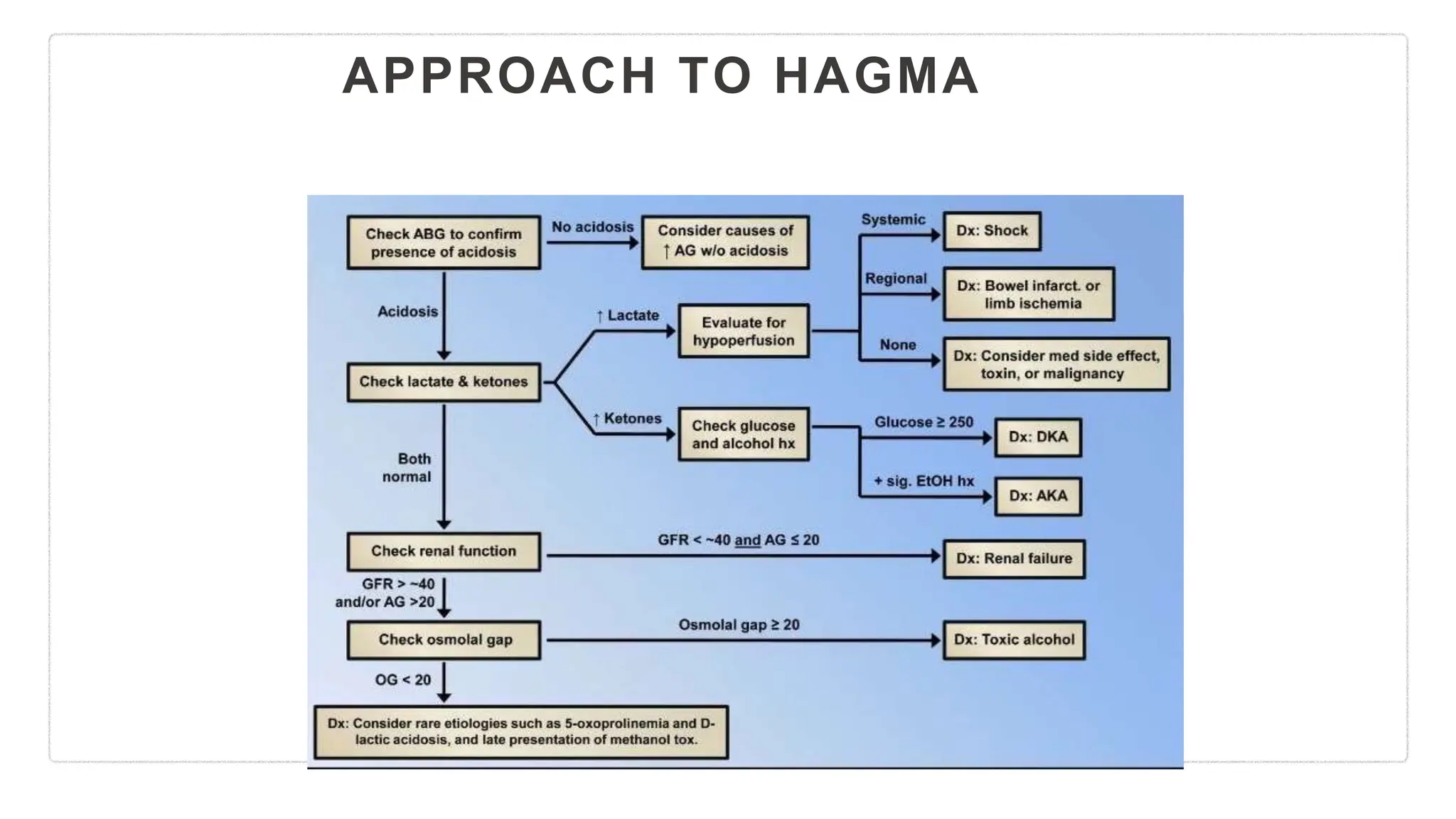
This document provides a comprehensive guide to interpreting arterial blood gases (ABG), focusing on acid-base balance, oxygenation, and ventilation status. It outlines assessment steps, compensation mechanisms for different acid-base disorders, and examples of both high and normal anion gap acidosis. The content includes critical formulas and equations for diagnosing respiratory and metabolic disorders, emphasizing the importance of systematic evaluation.


![CHECK FOR CONSISTENCY OF ABG
• Modified Henderson equation:[H+−][HCO3]/PaCO2 = 24
• Subtract the last two digits of the pH from 80; this value is
approximately equal to the H+ concentration .
• Example :pH: 7.42, pCO2: 30.8, HCO3- : 19.3, H+ : 38.1.
• 80 - last 2 digits of pH = 80-42 = 38 = approximately equal to measured
H + in the report.
• https://www.thoracic.org/professionals/clinical-resources/critical-care/clinical-education/abgs.php](https://image.slidesharecdn.com/abg-mixeddisorders-240206202111-26e99ccb/75/ABG-mixed-disorders-pptx-3-2048.jpg)