
![Said Jamal Eddin MD.SYRIA .Diaa Menem FRCS Libya
giasuddinahmadMS, DO,Bangladesh.. Rukban al saadi CES
KSA.Abdulkader Jamal eddin Medical Student.
NO FUNDS
Address for correspondence reprints:-
Name: SAID JAMAL EDDIN..BAISH G Hospital--JAZAN-KSA
Telephone: 00966505846293-00966558867848
Email: dr.jamal19.gmail.com
Conflicts of interest: No
Abstract;
Objective:
To explain a new surgical technique in squint surgery and to discuss and compare with old
Conventional ones
Background:
There is a taboo in all kinds of medicine which we did not discuss such as: squint surgical rules
and guidelines, Terms of ocular movements: -Antogisnt –Agonist –Yoke Muscle –Synergist,
Laws of ocular mobility: [Sherrington Law: reciprocal innervations] [Herring Law: equal
innervations] .A taboo such as conventional squint surgery and motility of the eye which we are
following many years. In my study and based on my observation and my experience I have
developed a new outstanding technique for squint surgery only depend on myectomy without
any suture with very good results. The classical surgical squint techniques mostly depend on
changing the mechanical action of the muscle. By resections or recessions .and those rules
explain the movement of the eye. I think the Eye is not a machine (turn to left and turn to right)...
There is also a compass like center in the eye ball or ocular muscles itself has control center like
pacemaker of the heart or there have been neurogenic control (supranuclear) of ocular muscles1
.
We don’t have any idea about these?!Or there may be another rule which need to discuss more.
1 Step by step squint surgery, Prasad Walimbe, first edition 2011](https://image.slidesharecdn.com/abstract0603-2-160318120104/75/Abstract-of-strabismus-surgery-2-2048.jpg)



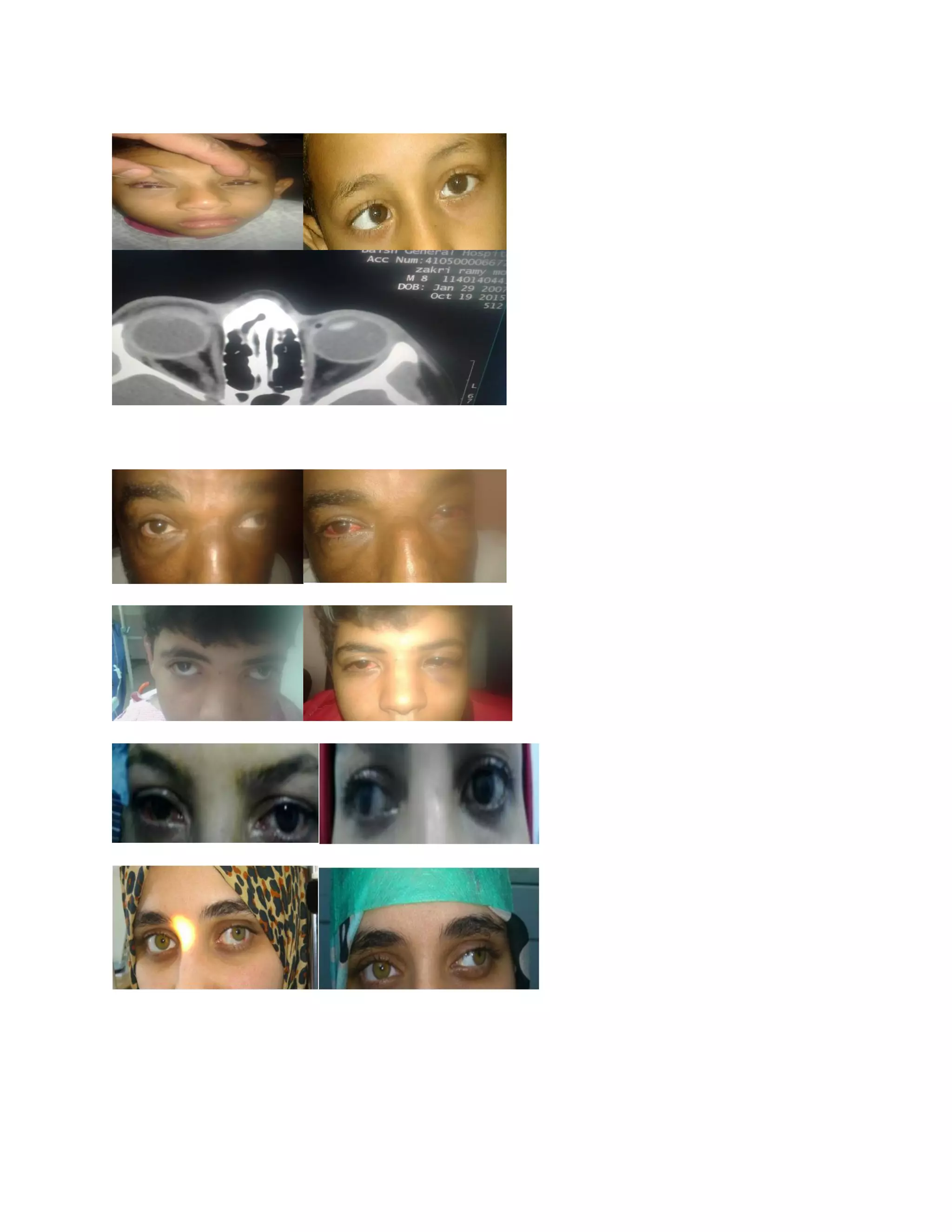


The document presents a new myectomy technique for squint surgery developed by Dr. Said Jamal Eddin, which eliminates the need for sutures and significantly shortens operative time while achieving excellent cosmetic and functional results. Based on observations of 74 squint patients, the technique reportedly allows the eye muscles to readjust naturally post-surgery, leading to minimal side effects and high rates of improvement in both alignment and binocular vision. This approach challenges traditional squint surgical methods by proposing a simpler, more efficient alternative that has shown promising outcomes in various cases.



































































