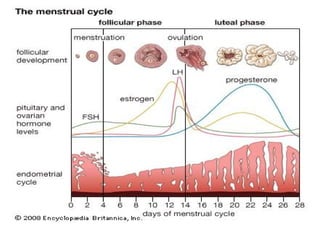
Menstrual Cycle
●Definition :cyclic uterine bleeding caused by
shedding of secretory endometrium
●Characteristics
●Menarche : the first menstrual period of
female(10-16 years old)
●Duration : 2-7 days
●Amount : 20-80ml
●Length : 3-5 weeks
●Cycle : 21-35 days
4.
Abnormal Bleeding fromGenital
Tract
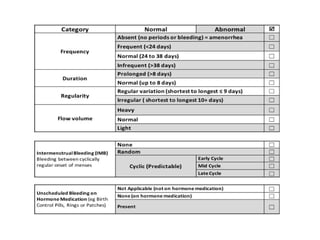
●Duration
●Menorrhagia - prolonged or excessive
uterine bleeding
●Hypomenorrhea - short or scanty uterine
bleeding
●Length of cycle
●Polymenorrhea - menstrual cycles < 21 days
●Oligomenorrhea - menstrual cycles > 35 days
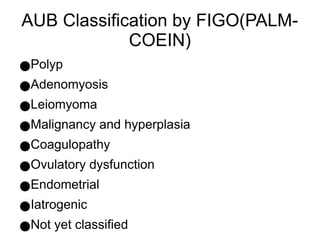
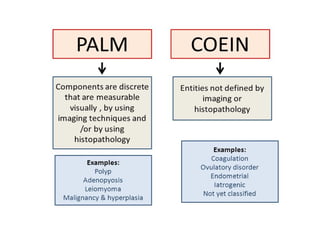
Endometrial polyps
●Localized overgrowthtissue, containing glands,
stroma, and blood vessels, covered with
epithelium
●Stimulated by estrogen
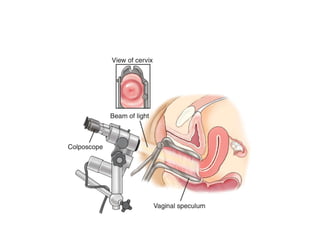
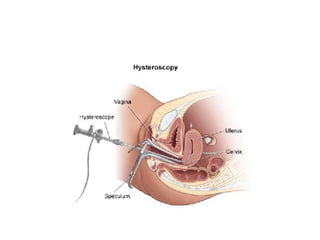
●Diagnosed by visualization and removal by
hysteroscopy
●Send for HPE to exclude malignancy
14.
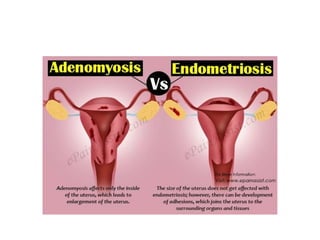
Adenomyosis
●Extension of endometrialglands and stroma in
the uterine myometrium
●Common in patient with multipara and history of
LSCS, D&C, and spontaneuous abortion
●Patient came with menorrhagia, secondary
dysmenorrhea and pressure symptoms
●Enlarged asymmetrical uterus on TAS
●Definite treatment by surgical intervention ie :
total abdominal hysterectomy
16.
Leiomyoma (Fibroids)
●Benign tumorsof the uterine myometrium
●Estrogen dependent
●Common in child bearing age, black, and
nulliparous
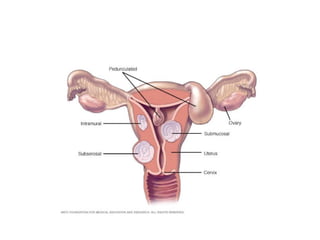
●Classified according to site : submucous,
intramural and subserous fibroids
●Can cause bleeding by increased vascularity of
uterus(red degeneration in pregnancy),
endometrial hyperplasia, ovarian congestion or
malignant changes
20.
●Most of fibroidsare asymptomatic that need no
intervention
●Intervention needed if give rise to symptoms
like bleeding, pain, infertility, and huge size that
lead to compressive symptoms
●Investigation by ultrasonography, HSG,
hysteroscopy and CT/MRI
●Definitine treatment are surgical intervention
●Myomectomy -want to keep uterus
●Hysterectomy -when myomectomy
contraindicated
21.
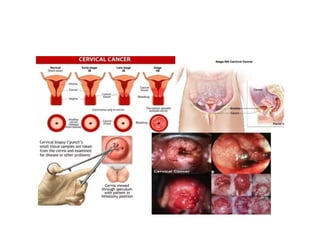
Malignancy
●Most common cancersin woman are cervical
and endometrial cancers
●Usually presented with painless PV bleed(coital
bleed or intermenstrual bleeding)
●Risk factors : prolonged exposure to
hyperestrogenic state
●Chronic anovulation
●PCOS
●Obesity
●Nulliparity
●Iatrogenic (on HRT)
22.
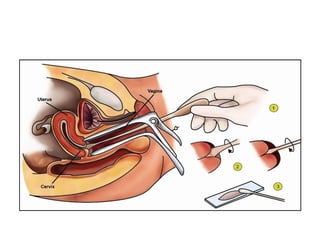
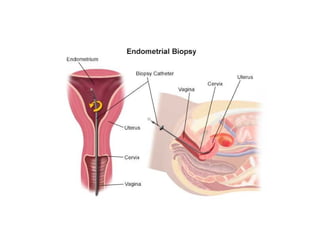
●Opportunistic screening bypap smear and
endometrial sampling in risky groups
●In highly suspicion of malignancy, for tumor
markers and imaging investigations
●Definite diagnosis by HPE
●Treatment by surgical, radiotherapy or
chemotherapy
28.
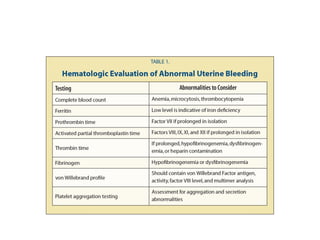
Coagulopathy
●Presence of bloodcoagulation disorder in
patients that lead to heavy menses
●Examples like von Willebrand disease,
prothrombin deficiency, leukemia, idiopathy
thrombocytopenic purpura, and hypersplenism
●May presented with epistaxis, bleeding gum or
ecchymosis
●Treat according to symptoms and causes
●Referral to hematologists
29.
Ovulatory dysfunction
●Alteration inneuroendocrine function
●Continuous estradiol production without corpus
luteum formation and progesterone production
thus causing excessive proliferation of
endometrium lead to necrosis
●Anovulatory bleeding commons in early years
after menarche due to immaturity of HPO axis
and perimenopausal woman due to lack of
synchronization of HPO
31.
●Anovulation causes by
●Extremesof reproductive life
●PCOS
●Hypothalamic dysfunction
●Abnormalities of other hormones(thyroid, prolactin,
and cortisol)
33.
Iatrogenic
●Abnormal uterine bleedingfrom medication
●Hyperprolactinemia from CNS dopamine
antagonism of drugs like risperidone
●COC and POP can cause breakthrough
bleeding
●Common meds like
●Selective estrogen receptor modulators(Tamoxifen)
●Gonadotropin releasing hormone agonists and
antagonists
34.
Endometrial
●Previously known asdysfunctional uterine
bleeding (DUB)
●Abnormal uterine bleeding not attributable to
any systemic cause or organic lesion in genital
tract
●Diagnosis of exclusion
●Classified into cyclic and acyclic
●Dysfunctional polymenorrhea due to short
proliferative or secretory phase
●Dysfunctional menorrhagia due to irregular ripening
or regular shedding
35.
Not Otherwise Specified
●Abnormalbleeding not in other classification
●Examples like foreign bodies or trauma
●Treatments are according to causes
36.
History
●Menstrual history likefrequency, duration and
amount of bleeding
●Pattern of menstruation
●Menstrual calendar to properly characterize
type of bleeding
●Ask about menarche, cycle length, menstrual
product, first day of LMP, contraceptives and
dysmenorrhea
●Inquire the bleeding of other systems like
epistaxis and gum bleeding
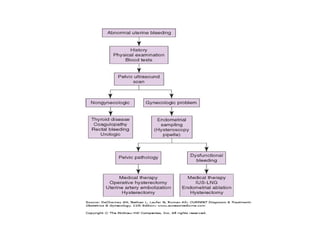
Management
●General management byABCD
●Correct anemia either by medication or blood
transfusion
●Maintain hemodynamic stability
●Correct the menstruation
●Prevent recurrence
●Prevent long term damage in anovulation
●Anemia, infertility, cancer
49.
Medical therapy
●High doseestrogen(temporary measure to stop
bleeding)
●Androgen(Danazol)
●Mirena(levonorgestrel intrauterine system)
●Progestin therapy
●Tranexamic acid
●NSAIDs
●COCP
50.
Reference
●Abnormal Uterine Bleedingin Comprehensive
Gynecology, 7th
edition
●Zagazig Textbook of Gynecology
●Obstetrics and Gynecology Malaysian Protocol