Normal physiology of
nerves:
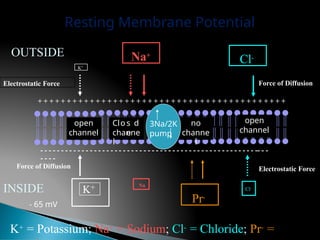
Differencein potential between the
inside and outside of a nerve
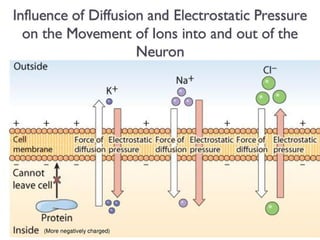
Difference in concentration of ions
inside and outside the plasma
membranes
4.
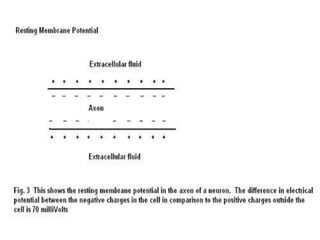
Polarized stage ofthe
membrane
Resting nerve is positive outside and
negative inside
Plasma membrane is not permeable
to sodium ions
Stimulation of nerveby the stimulus
Fall in the potential difference
Alteration in the permeability of the
membrane to sodium ions
Alteration in the concentration of ions
inside and outside the nerve membrane
Reversal of polarity
10.
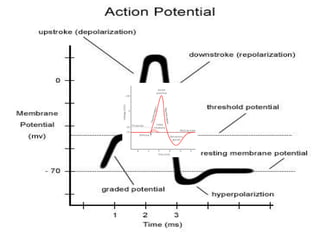
Phase 0
Stable restingpotential
When the cells are polarized and in an excitable state
awaiting a stimulus which will cause
depolarization
When a stimulus above the threshold potential strikes the
cell
the cell begins to depolarize.
Sodium ions rush into the cell causing the electrochemical
difference potential between the inside and outside of the
cell
to race toward zero
Phase 1
The depolarization phase
The electrochemical voltage change is so rapid that the
voltage overshoots the zero potential and tops out
around +20mV
Phase 1 is a very short phase where the potential difference
comes to rest near 0mV
11.
Phase 2
Plateau phase
Thetransmembrane action potential is maintained
near
0mV by the infusion of calcium ions.
The cell is in a depolarized state and restoration of the
resting membrane potential is beginning to take
place.
At the end of this phase, the cell begins to repolarize.
Phase 3
Rapid repolarization phase
The cell restores itself to the original polarized state of
-70mV
12.
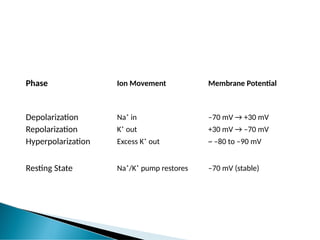
Phase Ion MovementMembrane Potential
Depolarization Na⁺ in –70 mV → +30 mV
Repolarization K⁺ out +30 mV → –70 mV
Hyperpolarization Excess K⁺ out ~ –80 to –90 mV
Resting State Na⁺/K⁺ pump restores –70 mV (stable)
13.
Adaptation of nervedue
to constant flow of
current
Unvarying current is not effective
in initiating an impulse
14.
Sensory nerve isstimulated the downward –traveling
impulse has no effect, but upward traveling impulse is
appreciated when it reaches brain
Sensory stimulation experienced varies with the duration
of the impulse
Long duration produce an uncomfortable, stabbing
sensation
Less duration produces less uncomfortable, stabbing
sensation
Impulses of 1ms and less produces a mild prickling
sensation
15.
The upward travelingimpulse is unable to pass the
first synapse, as it is traveling in the wrong direction,
but the downward-traveling impulse to the muscles
supplied by the nerves, causing them to contract
Stimulus applied to a motor trunk, impulses pass to
all the muscles that the nerve supplies below the
point at which it is stimulated, causing them to
contract
16.
Single stimulus simultaneouslyto a
number of motor units resulting in brisk
contraction, followed by immediate relaxation
If one stimulus is applied per second, each
produces an isolated contraction and there is
time for complete relaxation between the
impulses
17.
Increase frequency shortensthe periods
of relaxation
Frequency more than 20Hz there is no time
for complete relaxation between the
contraction_ resulting in partial tetany
Frequency more than 60Hz there is no
perceptible relaxation resulting in
full tetany
18.
Factors influences:
Numberof motor units activated
Intensity of current applied
Rate of change of current
If intensity of current suddenly rises there is
no time for accommodation to take place and
a muscle contraction results
19.
If thecurrent rises more slowly, there is some
accommodation and a greater intensity is
needed to produce a contraction
“An unpleasant sensory& emotional experience associated with
actual or potential tissue damage, or described in terms of such
damage” –
The International Association for the Study of Pain
Physiological response produced by activation of specific types of
nerve fibers
Experienced because of nociceptors being sensitive to extreme
mechanical, thermal, & chemical energy.
Composed of a variety of discomforts
🞂 Behavioral indicators of pain are crying, mood changes and from
facial expression.
23.
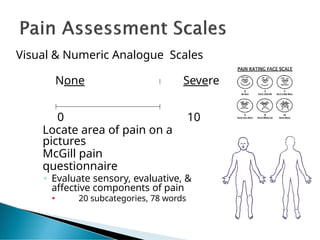
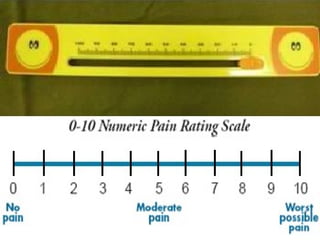
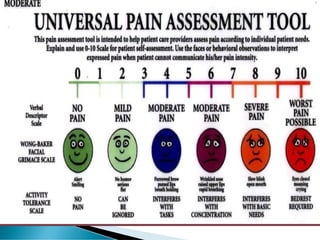
Visual & NumericAnalogue Scales
None Severe
0 10
Locate area of pain on a
pictures
McGill pain
questionnaire
◦ Evaluate sensory, evaluative, &
affective components of pain
🞄 20 subcategories, 78 words
24.
Does not interferewith most activities
Able to adapt to pain psychologically and with medication
or devices such as cushions
0 No pain
Feeling perfectly normal
1 (Very Mild):
Very light barely noticable pain
2 (Discomforting)
Minor pain, like lightly pinching the fold of skin between the
thumb and first finger with the other hand, using the fingernails
3 (Tolerable):
Very noticable pain, like an accidental cut, a blow to the nose
causing a
bloody nose, or a doctor giving you an injection
25.
Interferes with manyactivities, Interferes with many activities
Requires lifestyle changes but patient remains independent
4 Distressing
Strong, deep pain, like an average toothache, the initial pain from a
bee sting, or minor trauma to part of the body, such as stubbing your
toe real hard
5 Very Distressing
Strong, deep, piercing pain, such as a sprained ankle when you stand
on it
wrong, or mild back pain
6 Intense
At this point you begin to have trouble holding a job or
maintaining normal social relationships
26.
Unable to engagein normal activities
Patient is disabled and unable to function independently
7- VeryIntense
The pain completely dominates your senses, causing you
to think unclearly about half the time
8 Utterly Horrible
Pain so intense you can no longer think clearly at all, and
have often undergone severe personality change if the pain
has been present for a long time
27.
9 Excruciating
Unbearable
Pain sointense you cannot tolerate it and demand pain
killers or surgery, no matter what the side effects or risk
10 Excruciating
Those who have suffered a severe accident, such as a
crushed hand, and lost consciousness as a result of the
pain and not blood loss, have experienced level 10.
Pain so intense you will go unconscious shortly
30.
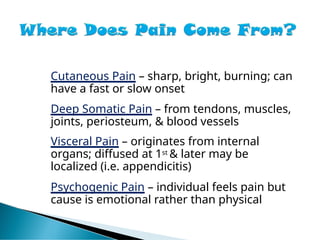
Cutaneous Pain –sharp, bright, burning; can
have a fast or slow onset
Deep Somatic Pain – from tendons, muscles,
joints, periosteum, & blood vessels
Visceral Pain – originates from internal
organs; diffused at 1st & later may be
localized (i.e. appendicitis)
Psychogenic Pain – individual feels pain but
cause is emotional rather than physical
31.
Fast vs. SlowPain –
◦ Fast – localized; carried through A-delta axons in
skin
◦ Slow – aching, throbbing, burning; carried by C
fibers
◦ Nociceptive neuron transmits pain info to
spinal cord via unmyelinated C fibers &
myelinated A-delta fibers.
🞄 The smaller C fibers carry impulses @ rate of 15
pulses/sec.
🞄 The larger A-delta fibers carry impulses @ rate of 40
pulses/sec.
32.
Types of Nerves
NEUROTRANSMITTERS:
CHEMICALSUBSTANCES THAT ALLOW
NERVE IMPULSES TO MOVE FROM ONE
NEURON TO ANOTHER
Found in synapses
◦ Substance P - thought to be
responsible for the transmission of
pain-producing impulses
33.
Afferent (Ascending) –transmit impulses
from the periphery to the brain
◦ First Order neuron
◦ Second Order neuron
◦ Third Order neuron
Efferent (Descending) – transmit impulses
from the brain to the periphery
34.
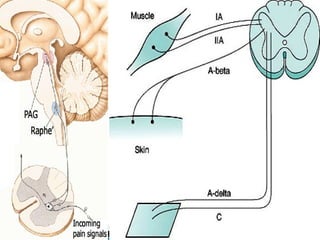
Stimulated by sensoryreceptors
End in the dorsal horn of the spinal Cord
Fiber Type Carries... Speed
A-beta Touch, pressure Fast
A-delta Sharp pain Medium
C fibers Dull, aching pain Slow
36.
Descending Pain Modulation(Descending Pain
Control Mechanism)
Transmit impulses from the brain (corticospinal
tract in the cortex) to the spinal cord (lamina)
◦ Periaquaductal Gray Area (PGA) – release Enkephalins
◦ Nucleus Raphe Magnus (NRM) – release Serotonin
◦ The release of these neurotransmitters inhibit
ascending neurons
Stimulation of the PGA in the midbrain & NRM in the
pons & medulla causes analgesia.
Endogenous opioid peptides - Endorphins &
Enkephalins
38.
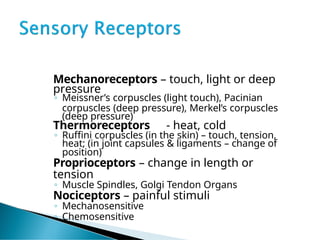
Mechanoreceptors – touch,light or deep
pressure
◦ Meissner’s corpuscles (light touch), Pacinian
corpuscles (deep pressure), Merkel’s corpuscles
(deep pressure)
Thermoreceptors - heat, cold
◦ Ruffini corpuscles (in the skin) – touch, tension,
heat; (in joint capsules & ligaments – change of
position)
Proprioceptors – change in length or
tension
◦ Muscle Spindles, Golgi Tendon Organs
Nociceptors – painful stimuli
◦ Mechanosensitive
◦ Chemosensitive
39.
Sensitive to repeatedor prolonged
stimulation
Mechanosensitive – excited by stress
& tissue damage
Chemosensitive – excited by the
release of chemical mediators
◦ Bradykinin, Histamine,
Prostaglandins, Arachadonic Acid
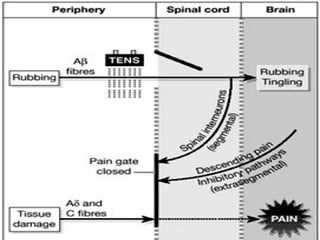
Not all painsignals pass freely to the brain. The spinal cord
acts like a gate—sometimes letting the signals through,
sometimes blocking or reducing them.
Where is this gate?
Located in the dorsal horn of the spinal cord (specifically in
an area called substantia gelatinosa).
When the "gate" is closed:
Non-painful stimuli (like rubbing, vibration, TENS) activate A-beta fibers.
These fibers inhibit pain signals from A-delta and C fibers.
So the pain signal is reduced or blocked from reaching the brain.
42.
When the "gate"is open:
Pain fibers (A-delta & C) dominate.
The gate allows pain signals to pass freely to the brain.
You feel more intense pain
Brain’s Role:
The brain can also influence the gate:
If you're anxious, stressed, or focused on the pain, the gate may open wider.
If you're relaxed, distracted, or using coping strategies, the gate can close more.
Everyday Example:
You hit your elbow → it hurts (pain fibers activated).
You rub it → rubbing stimulates A-beta fibers → gate closes → pain decreases.
That’s Gate Control in action.
43.
Applications in Therapy:
Thetheory explains why modalities like these work:
TENS (Transcutaneous Electrical Nerve Stimulation)
Massage
Heat and cold therapy
Rubbing or applying pressure
They activate A-beta fibers and help "close the gate" to
pain.
44.
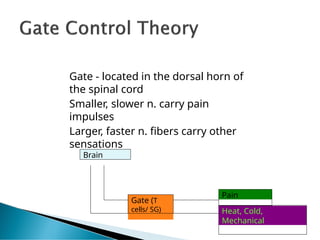
Gate - locatedin the dorsal horn of
the spinal cord
Smaller, slower n. carry pain
impulses
Larger, faster n. fibers carry other
sensations
Brain
Pain
Heat, Cold,
Mechanical
Gate (T
cells/ SG)
45.
The Central BiasingTheory explains how the brain itself can
influence and reduce pain by sending signals down the
spinal cord to inhibit incoming pain messages.
Where does this happen?
• Begins in higher brain centers (like the cortex, limbic system, hypothalamus)
• Sends signals down to the periaqueductal gray (PAG) in the midbrain
• Then to the raphe nucleus in the medulla
• And finally to the spinal cord (dorsal horn), where it inhibits pain transmission
46.
How does itreduce pain?
The descending pathway releases natural painkillers like:
Endorphins
Enkephalins
Serotonin
Norepinephrine
These chemicals:
Block or reduce the release of substance P (a neurotransmitter that
carries pain)
Inhibit pain-carrying neurons in the spinal cord
47.
Least understood ofall the theories
🞂 Stimulation of A-delta & C fibers causes release
of B-endorphins from the PAG & NRM
Or
ACTH/B-lipotropin is released from the anterior
pituitary in response to pain – broken down into
B-endorphins and corticosteroids
Mechanism of action – similar to enkephalins to
block ascending nerve impulses
Examples: TENS (low freq. & long
pulse duration)