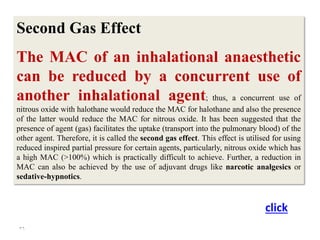
The document discusses the history and principles of general anesthesia, highlighting the contributions of Ibn al-Quff and the evolution of anesthetic practices. It details the stages of anesthesia, factors influencing anesthetic selection, and the physiological effects of various anesthetic agents. Additionally, it explains the mechanisms of action, types of anesthesia such as neuroleptanalgesia and dissociative anesthesia, along with their applications and potential adverse effects.


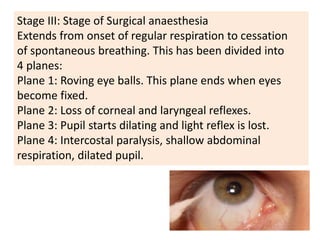
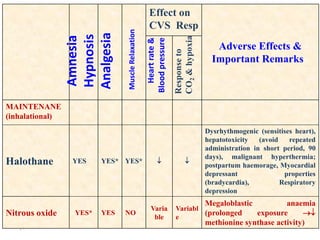
![Stages of Anaesthesia [Depth of Anesthesia]
These stages were defined for the original anesthetic
Ether, which produces a slow onset of anesthesia.
With modern anesthetics, the stages merge because
of the rapid onset of stage III.](https://image.slidesharecdn.com/8963-241020221909-7b69c1a8/85/8hyjhhcdgydgyuguidhiudcgiudcgiudgcdu963-pdf-12-320.jpg)
















![GENERAL_ANAESTHETICS[1] - Read-Only.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/generalanaesthetics1-read-only-241121061647-7b143b40-thumbnail.jpg?width=640&height=640&fit=bounds)





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






