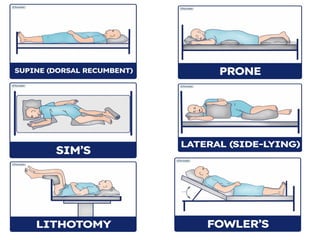
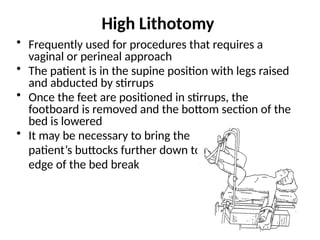
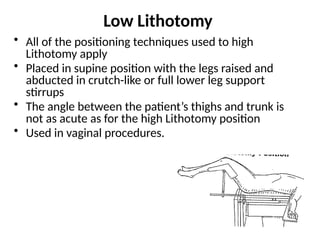
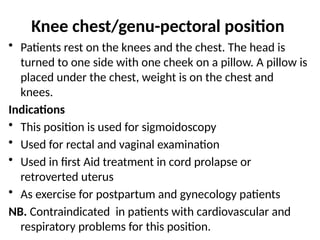
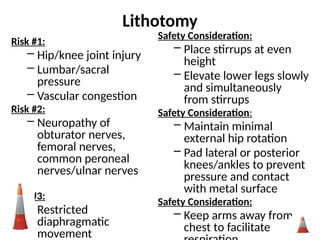
The document outlines the definition, purpose, principles, and procedures for proper patient positioning in healthcare. It discusses various positions like supine, prone, lateral, and lithotomy, along with their indications, contraindications, and safety considerations to promote patient comfort and prevent complications. It emphasizes the importance of proper assessment, documentation, and the need for collaboration and safety measures during positioning.












































![DATA_COLLECTION_METHODS by htc student [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/datacollectionmethods1-250417191022-4550b3ec-thumbnail.jpg?width=640&height=640&fit=bounds)























