Download as PDF, PPTX
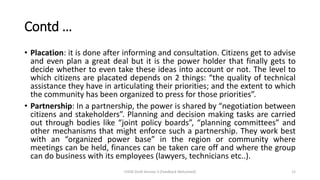
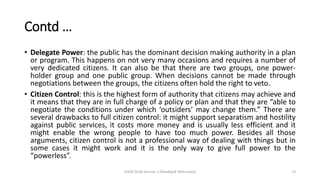
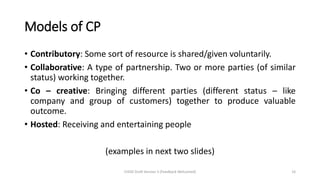
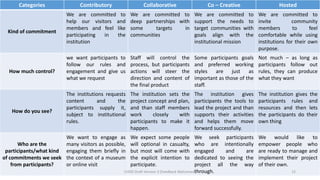
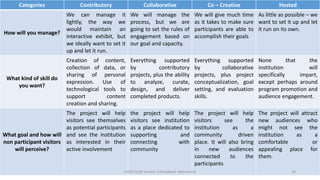
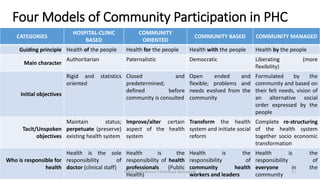

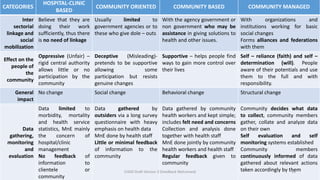
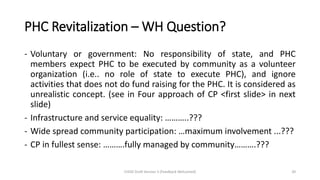



This document discusses community participation in community health services. It defines participation as involvement or engagement of community members. There are different forms and levels of participation, from passive participation where communities are involved as a means to achieve predetermined objectives, to active participation where communities take responsibility for their own development. The objectives, importance, and different levels of community participation in health are described, including compliance, collaboration, and local control. Models of participation discussed include contributory, collaborative, co-creative, and hosted participation.































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













