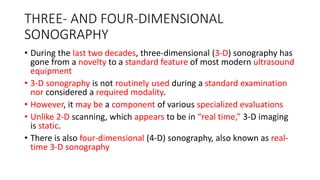
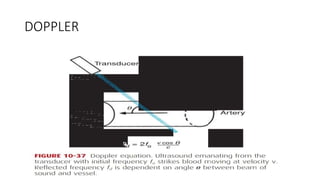
3D and 4D sonography provide static or real-time 3D views of the fetus, respectively, but are not routinely used in standard exams. Doppler ultrasound evaluates blood flow in various fetal vessels like the umbilical artery, ductus arteriosus, uterine artery, middle cerebral artery, and ductus venosus to monitor fetal well-being. Abnormal flow patterns in these vessels can indicate conditions like fetal growth restriction. Fetal MRI provides superior anatomical images compared to ultrasound and can help further characterize abnormalities, guide fetal therapy, or assess complications in high-risk pregnancies.




















![Umbilical artery doppler [1]](https://cdn.slidesharecdn.com/ss_thumbnails/umbilicalarterydoppler1-210517112207-thumbnail.jpg?width=640&height=640&fit=bounds)































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















