Downloaded 23 times
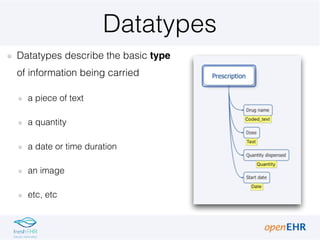
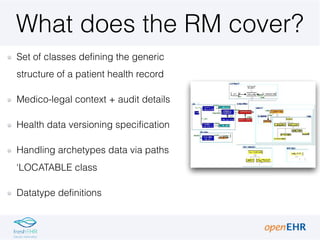
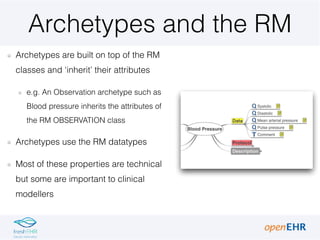
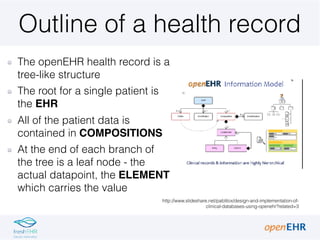
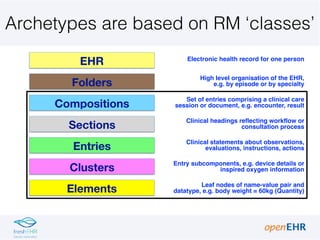
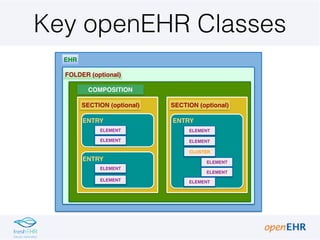
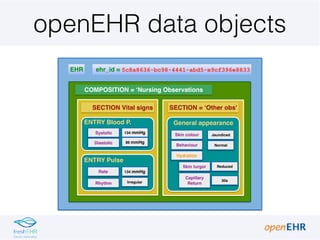
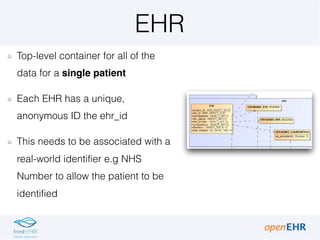
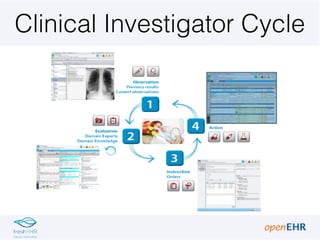
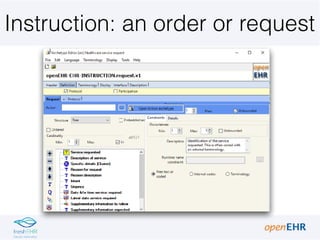
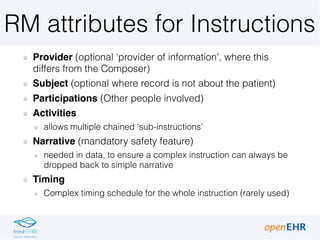
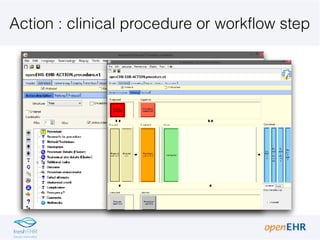
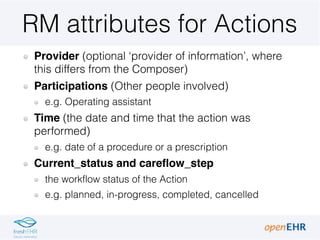
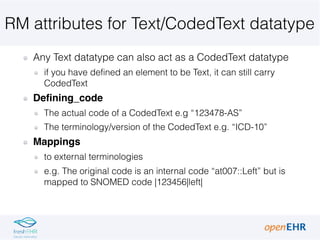



The document provides an introduction to key concepts in the openEHR Reference Model (RM) including: 1) It describes several core RM classes - EHR, Composition, Section, and Entry - that define the structure of a patient health record in openEHR. Compositions contain patient data organized into Sections and Entries. 2) It explains key attributes for different types of Entries defined in the RM like Observations, Evaluations, Instructions, and Actions that support the "clinical investigator cycle". 3) It outlines important datatypes in the RM like Quantity, Text, and CodedText and their relevant attributes for modeling clinical data values and coded items. 4) It describes how archetypes are