Download as PDF, PPTX
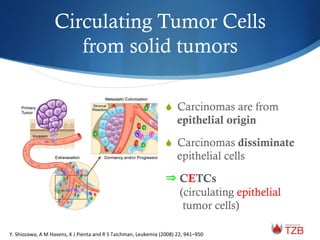

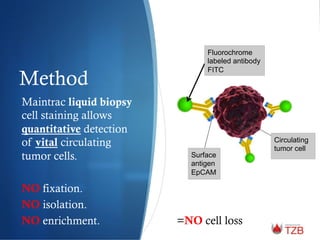
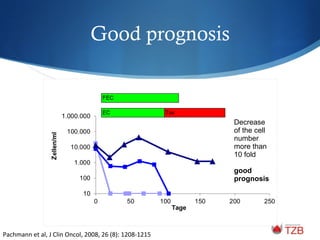
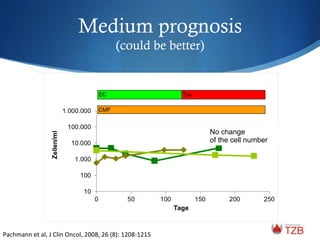
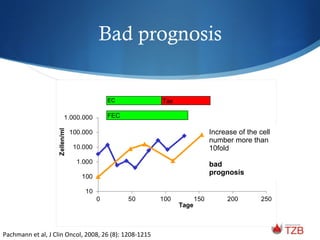
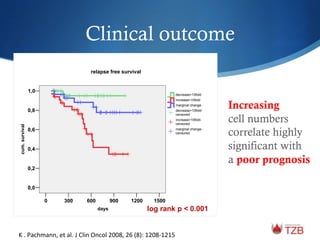


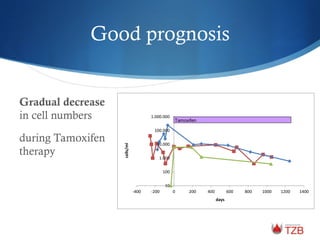
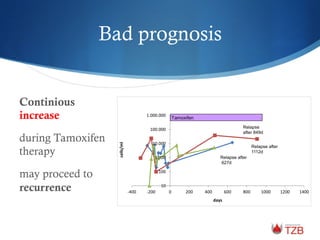
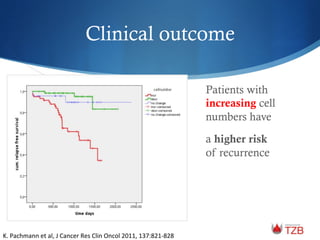
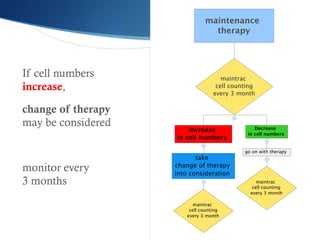

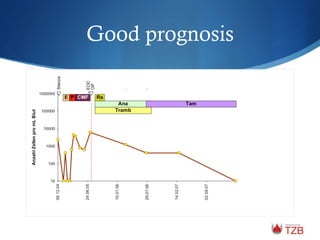
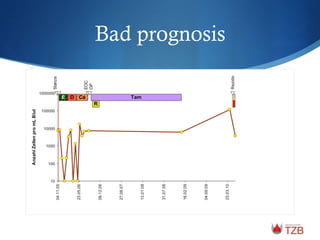
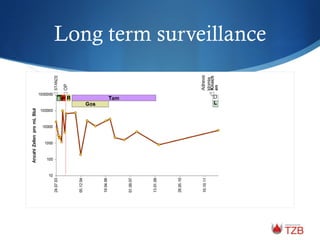
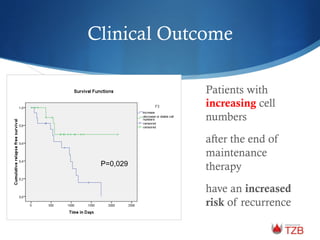
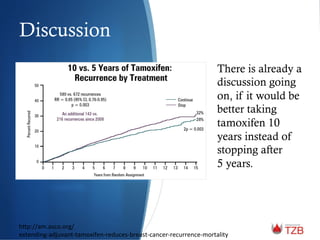
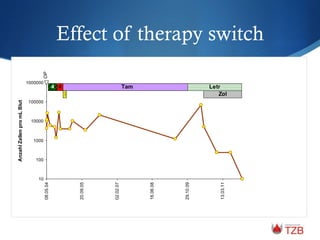
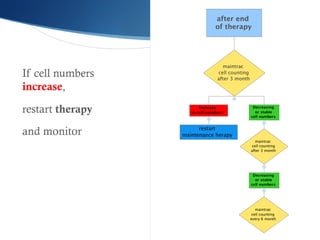


The document discusses maintrac®, a tool for monitoring therapy success in solid tumors through the analysis of circulating epithelial tumor cells (CETCs) in nonmetastatic primary breast cancer patients. It highlights the correlation between the number of CETCs and patient prognosis, identifying that a significant increase in CETCs at the end of treatment may predict relapse. The study emphasizes the potential of CETC monitoring to adjust treatment strategies, improving patient outcomes by providing early warnings of potential relapse.


































![3 minute talk July 2014 [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/92aade0e-712d-439b-8308-1fa937f77fa7-160106000704-thumbnail.jpg?width=640&height=640&fit=bounds)


















































