Downloaded 13 times
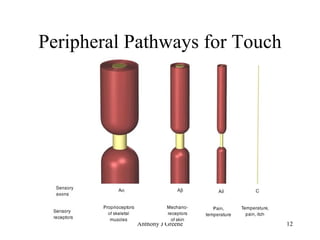
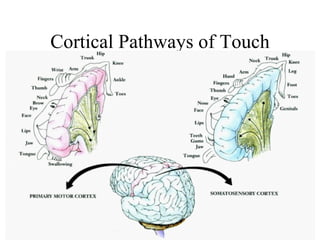
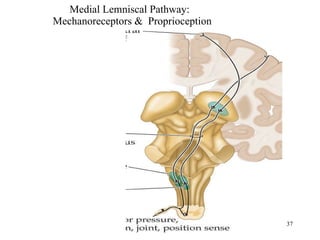

Touch is the oldest sense and involves mechanoreceptors in the skin that detect deformations. There are four main receptor types - Meissner corpuscles, Pacinian corpuscles, Merkel disks, and Ruffini endings. Tactile information is processed in the peripheral and central nervous systems, with different cortical areas representing information from different body parts. Proprioception provides information about body position and movement through receptors in the muscles and joints. Haptics and proprioception together allow us to identify objects and perceive their location through active touch.