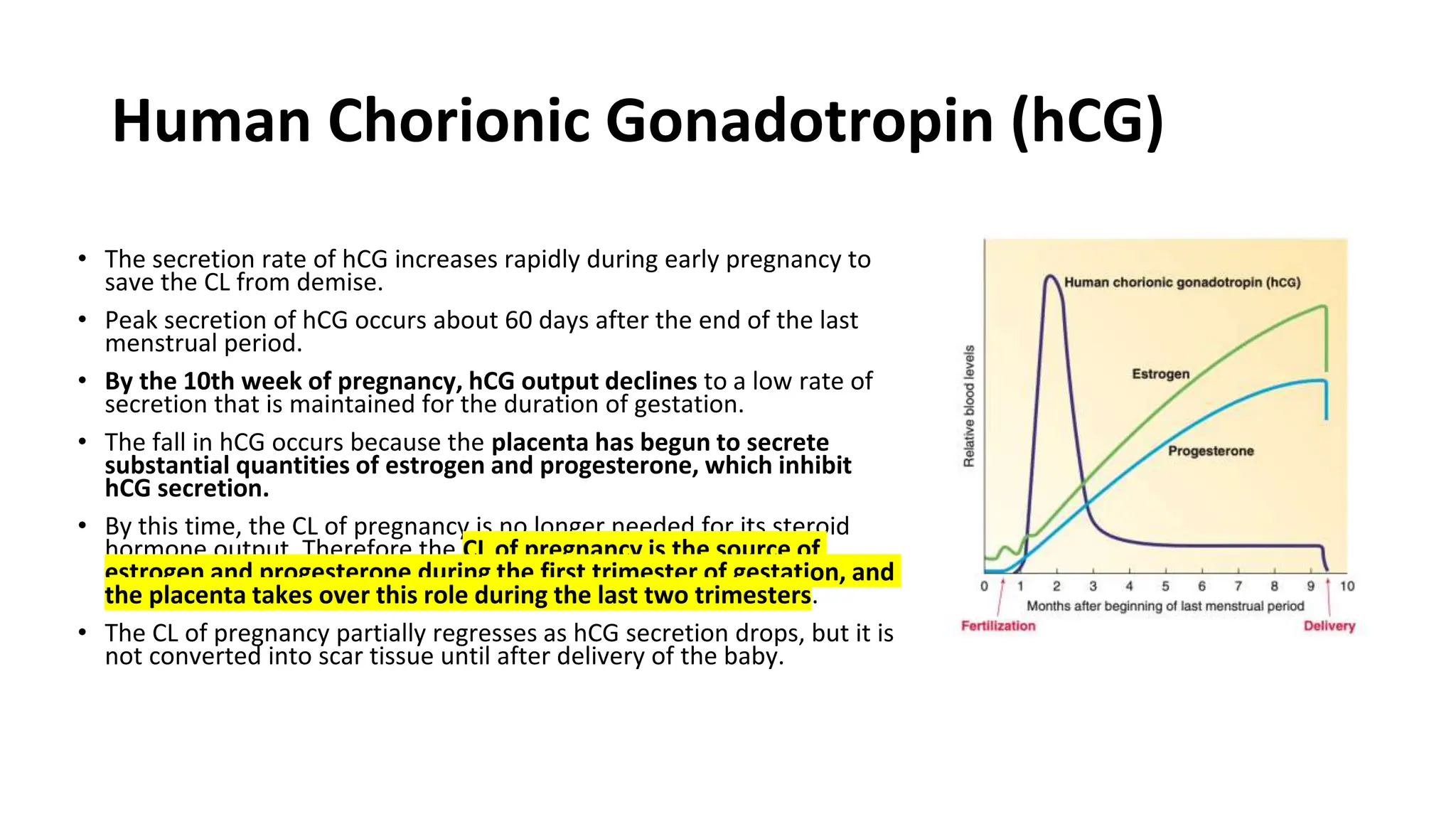
The document summarizes key stages of human fertilization and early pregnancy development. It describes how the ovum is transported to the oviduct where fertilization occurs with sperm. It then discusses early embryo development through the morula and blastocyst stages. It explains implantation of the blastocyst in the uterine lining and the subsequent development of the placenta and amniotic sac to support the growing embryo and fetus. The roles of hormones like hCG in supporting early pregnancy are also outlined.