SELECTIVE TOXICITY
Selectivetoxicity refers to the ability of the drug to targets sites that are relative
specific to the microorganism responsible for infection
Sometimes these sites are unique to the microorganism or simply more essential
to survival of the microorganism than to the host.
4.
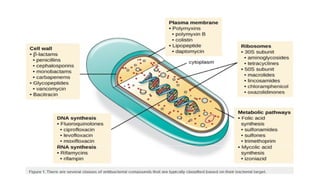
Examples of suchspecific or relatively specific sites include:
specific fungal or bacterial cell wall synthesizing enzymes
The bacterial ribosome
machinery of viral replication.
This explains how drugs inhibit cell wall biosynthesis, protein synthesis,
membrane function, nucleic acid synthesis, and metabolic pathways
and thus exert their intended/desired effects
6.
Resistance :-
• WHO- Defines as micro-organisms that are not inhibited by usually
achievable systemic concentration of an antimicrobial agent(AMA)
with normal dosage schedule and / or fall in the minimum
inhibitory concentration (MIC) range.
• When a species is subjected to chemical warfare, that threatens
its extinction it often evolves mechanisms to survive under that
stress development of resistance.
7.
• Two majorfactors are associated with emergence of
antibiotic
resistance:
- Evolution
- Clinical/ Environmental practices.
8.
NATURAL
RESISTANCE :-
• Somemicrobes lack the metabolic process or the target site
for particular drug.
• e.g: - Gram-negative bacilli are normally unaffected by
penicillin G
- M. tuberculosis is insensitive to tetracyclines.
• This resistance does not pose a significant clinical problem.
9.
ACQUIRED
RESISTANCE :-
• Itis the development of resistance by an organism (which
was sensitive before) due to the prolonged use of an AMA.
• Some bacteria are notorious for rapid acquisition of
resistance
e.g. staphylococci, coliforms, tubercle bacilli.
10.
RESISTANCE
MECHANISMS :-
BIOCHEMICALMECHANISMS -
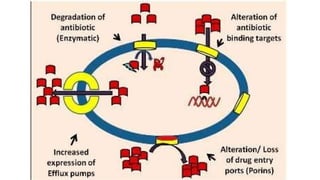
•Antimicrobial resistance can develop at any one or more of steps
in the process
• Reduced entry of antibiotic into pathogen
• Enhanced export of antibiotic by efflux pumps
• Release of microbial enzymes that destroy the antibiotic
11.
• Alteration ofmicrobial proteins that transform pro-drugs to
the
effective moieties
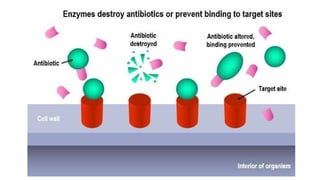
• Alteration of target proteins
• Development of alternative pathways to those inhibited by
the antibiotic
13.
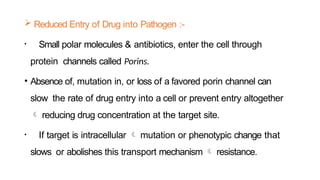
Reduced Entryof Drug into Pathogen :-
• Small polar molecules & antibiotics, enter the cell through
protein channels called Porins.
• Absence of, mutation in, or loss of a favored porin channel can
slow the rate of drug entry into a cell or prevent entry altogether
reducing drug concentration at the target site.
• If target is intracellular mutation or phenotypic change that
slows or abolishes this transport mechanism resistance.
14.
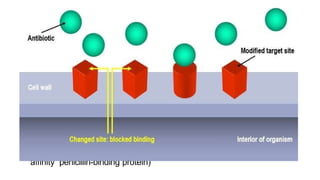
Resistance Dueto Reduced Affinity of Drug to Altered Target
Structure :-
• A reduced affinity of drug for its target or the enzyme that
converts the prodrug to active drug. Such alterations may be due to
Mutation of the natural target (e.g., fluoroquinolone resistance)
Target modification (e.g., ribosomal protection type of resistance
to macrolides and tetracyclines)
Acquisition of a resistant form of the native, susceptible target (e.g.,
staphylococcal methicillin resistance caused by production of a low-
affinity penicillin-binding protein)
15.
• Examples :-
•The penicillin-resistant gonococci are less permeable to penicillin
G.
• Chloroquine-resistant P
. Falciparum accumulates less chloroquine.
16.
ResistanceDue toDrug Efflux :-
• Microorganisms can over-express efflux pumps and then
expel antibiotics to which their susceptible.
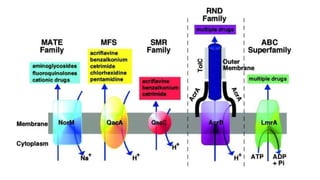
• Five major systems of efflux pumps
- The multidrug and toxic compound extruder (MATE)
- The major facilitator superfamily (MFS) transporters
- The small multidrug resistance (SMR) system
- The resistance nodulation division (RND) exporters
- A
TPbinding cassette (ABC) transporters
18.
• Drug resistanceto erythromycin, fluoroquinolones & Anti-
malarial drugs are mediated through these Efflux pumps.
19.
Resistance Dueto Destruction of Antibiotic :-
• Drug inactivation is a common mechanism of drug resistance.
• Bacterial resistance to aminoglycosides aminoglycoside-
modifying enzyme
• β -lactam antibiotics β -lactamase
21.
Hetero-resistance andViral Quasi Species :-
• It is said to be present when only a subset of the total
microbial population is resistant.
• Increased therapeutic failures and mortality is seen.
• Viral evolution due to drug and immune pressure Quasi
species.
• Quasi species (eg.HIV-1&HIV-2) are resistant to antiretroviral
agents failure of antiretroviral therapy.
22.
Resistance dueto Enhanced Excision of incorporated drug :-
• These drugs are incorporated into the viral DNA chain and cause chain
termination.
• E.g. NRTIs such asAZT are 2′-deoxyribonucleoside analogs
5′-triphosphate and compete with natural nucleotides.
23.
MUTATION –
•Mutation and antibiotic selection of the resistant mutant are
the molecular basis for development of resistance in many
bacteria, viruses, and fungi.
• Mutations are not caused by drug exposure. They occur as a
survival advantage, when drug is present.
24.
• Mutations mayoccur in the gene encoding
(1) The target protein, altering its structure so that it no longer
binds the drug
(2)Aprotein involved in drug transport
(3)Aprotein important for drug activation or inactivation
(4)In a regulatory gene or promoter gene affecting expression of
the target, a transport protein, or an inactivating enzyme
25.
• Suboptimal dosingstrategies selective kill of the more
susceptible population, which leaves the resistant isolates to
flourish.
• Asingle-step mutation high degree of resistance.
• The Multi-step mutation clinically significant resistance.
• E.g : Combination of pyrimethamine and sulfadoxine inhibits
Plasmodium falciparum’s folate biosynthetic pathway via inhibition
of dihydrofolate reductase (DHFR) by pyrimethamine and
dihydropteroate synthetase (DHPS) by sulfadoxine.
26.
Hypermutable Phenotypes:-
• The ability to protect genetic information from disintegrating and
also to be flexible enough to allow genetic changes.
• This is accomplished principally by the
- Insertion of the correct base pair by DNApolymerase III
- Proofreading by the polymerase
- Postreplicative repair.
• Mutator (Mut) phenotypes antibiotic resistance .
27.
Quorum
sensing :-
• Microbescommunicate with each other and exchange signaling
chemicals (Autoinducers) coordinate gene expression for
virulence, conjugation, apoptosis, mobility and resistance.
• QSsignal molecules AHL, AIP
, AI-2 & AI-3 have been identified
in GM-ve bacteria
• Gram-positive bacteria use processed oligo-peptides
to communicate.
28.
• Several QSinhibitorsmolecules have been synthesized AHL,
AIP
, and AI-2 analogues Potent Virulence inhibitors.
• QScontrols virulence factor production in Gram-positive human
pathogens including S. aureus, Listeria monocytogenes,
Enterococcus faecalis, and Clostridium perfringens
• V. cholera, P. aeruginosa Gram negative bacteria .
29.
GENETRANSFER :-
•Drug resistance may be acquired by passage of the trait vertically
to daughter cells, but more commonly it is acquired by horizontal
transfer of resistance by,
- Transduction
- Transformation
- Conjugation
30.
• Horizontal transferof resistance genes is greatly facilitated
by Mobile genetic elements
Plasmid
s
Transducin
g phages
Transposabl
e
elements
Integrons Gene
cassette
s
Insertion
sequences
Transposons Transposable
phages
31.
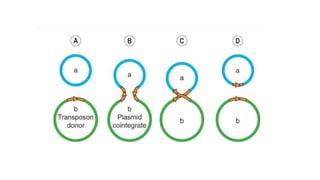
• Insertion sequencesdo not encode resistance, but they function
as sites for integration of other resistance-encoding elements.
• Transposons are insertion sequences that also code for
drug resistance & other function.
• Transposon move between chromosome and plasmid thus
“hitchhike” the resistant gene out of the host and into a
recipient.
32.
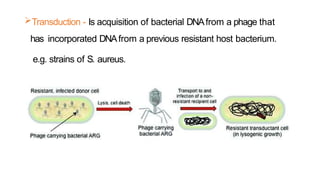
Transduction - Isacquisition of bacterial DNAfrom a phage that
has incorporated DNAfrom a previous resistant host bacterium.
e.g. strains of S. aureus.
33.
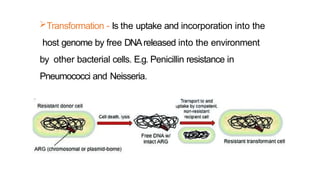
Transformation - Isthe uptake and incorporation into the
host genome by free DNAreleased into the environment
by other bacterial cells. E.g. Penicillin resistance in
Pneumococci and Neisseria.
34.
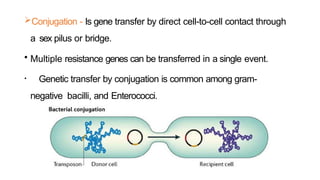
Conjugation - Isgene transfer by direct cell-to-cell contact through
a sex pilus or bridge.
• Multiple resistance genes can be transferred in a single event.
• Genetic transfer by conjugation is common among gram-
negative bacilli, and Enterococci.
36.
CROSS
RESISTANCE :-
• Acquisitionof resistance to one AMA conferring resistance
to another AMA to which the organism has not been
exposed
e.g. - resistance to one sulfonamide means resistance to all
others,
-resistance to one tetracycline means insensitivity to all
others
• Partial cross resistance is sometimes seen in unrelated
drugs
37.
• Cross resistancemay be
Two-way, e.g. between erythromycin and clindamycin and vice
versa
One-way, e.g. development of neomycin resistance by
enterobacteriaceae makes them insensitive to streptomycin but
many streptomycin-resistant organisms remain susceptible to
neomycin.
38.
Prevention of drug
resistance:-
No indiscriminate and inadequate or unduly prolonged use of
AMAs should be made.
Prefer rapidly acting and selective (narrow spectrum) AMAs.
Use combination of AMAs for prolonged therapy e.g. tuberculosis,
SABE.
Intensive treatment for notorious organisms.










































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










