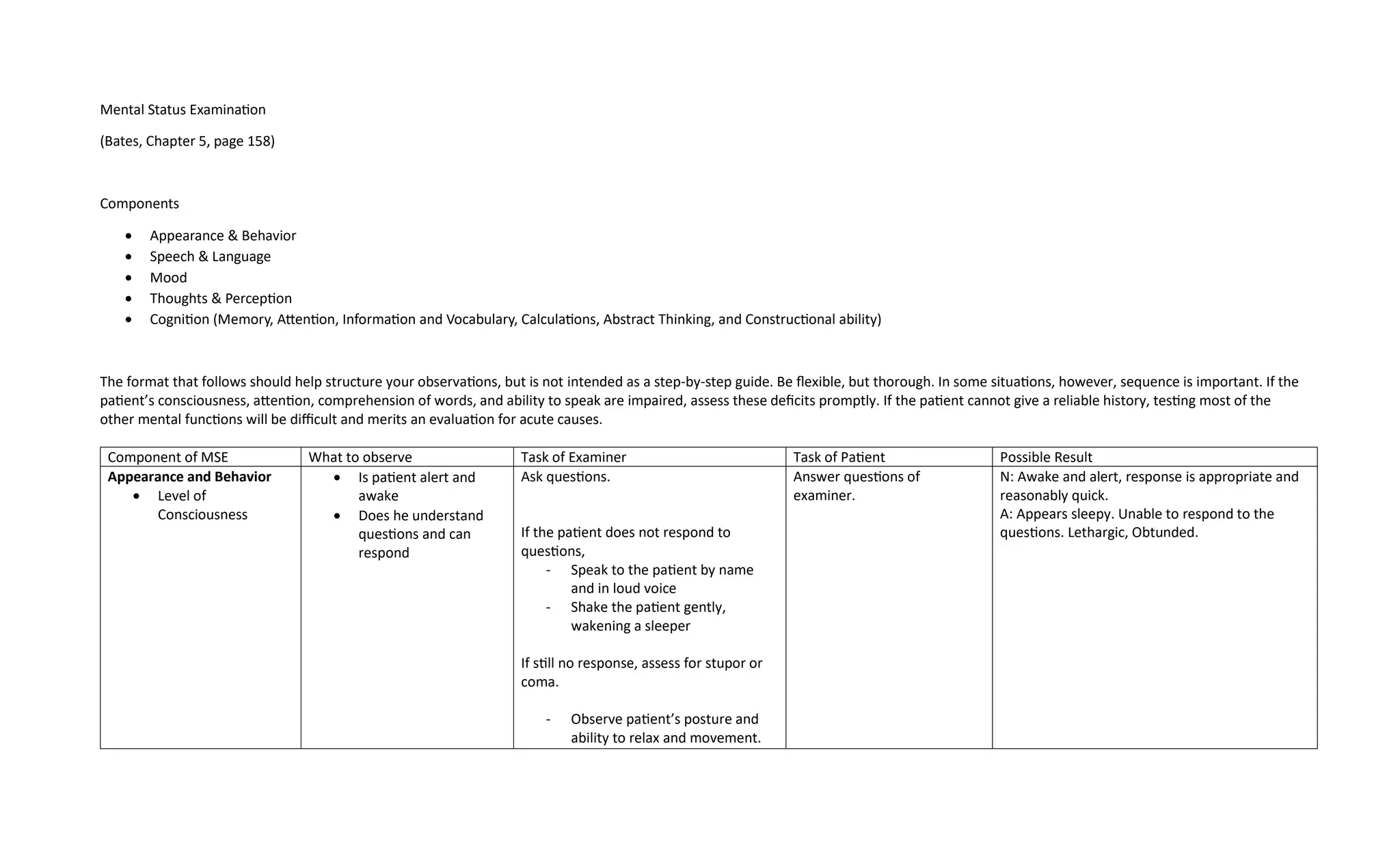
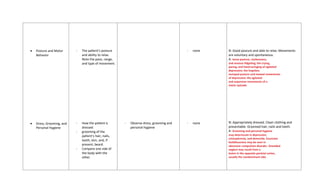
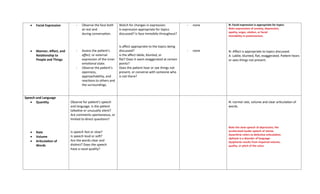
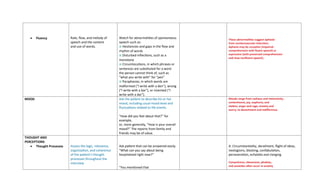
The document outlines the components of a mental status examination (MSE) including observations of appearance, behavior, speech, mood, thoughts, and cognitive functions. It provides a structured approach for examiners to assess and document various mental health indicators, emphasizing flexibility while ensuring thoroughness. Each component details what to observe, the tasks for both the examiner and the patient, and possible results to help diagnose mental health conditions.