Downloaded 18 times

![• EBWater 23 litres
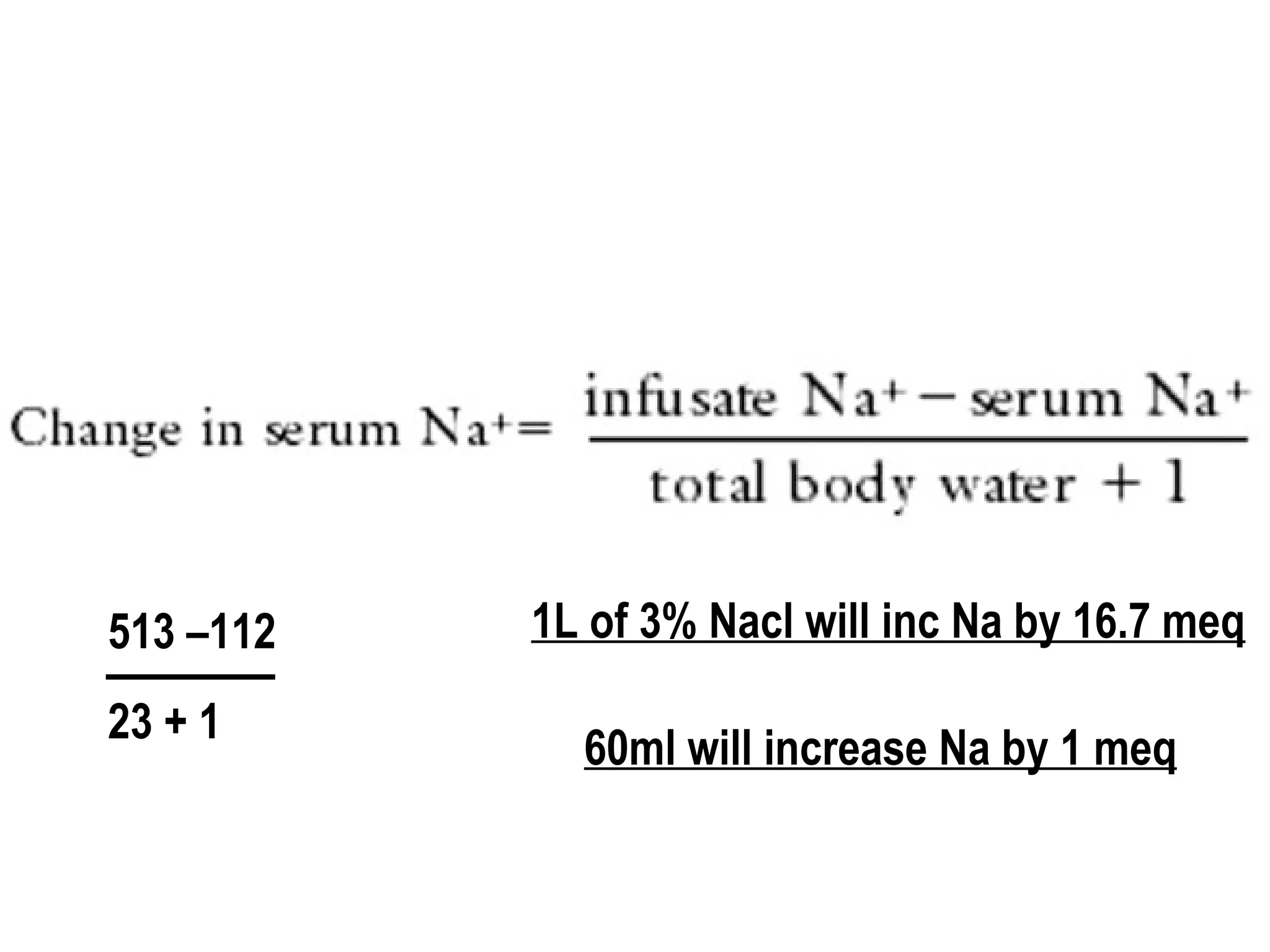
Na now 112 x 23
If you give 1L of 3% saline
(513 x 1) + (112x 23)
New conc of Na = (513 x 1) + (112x 23)/24
diff of Na = [(513 x 1) + (112x 23)/24] – (112)](https://image.slidesharecdn.com/08-140422135109-phpapp01/75/08-fluid-and-electrolytes-24-2048.jpg)
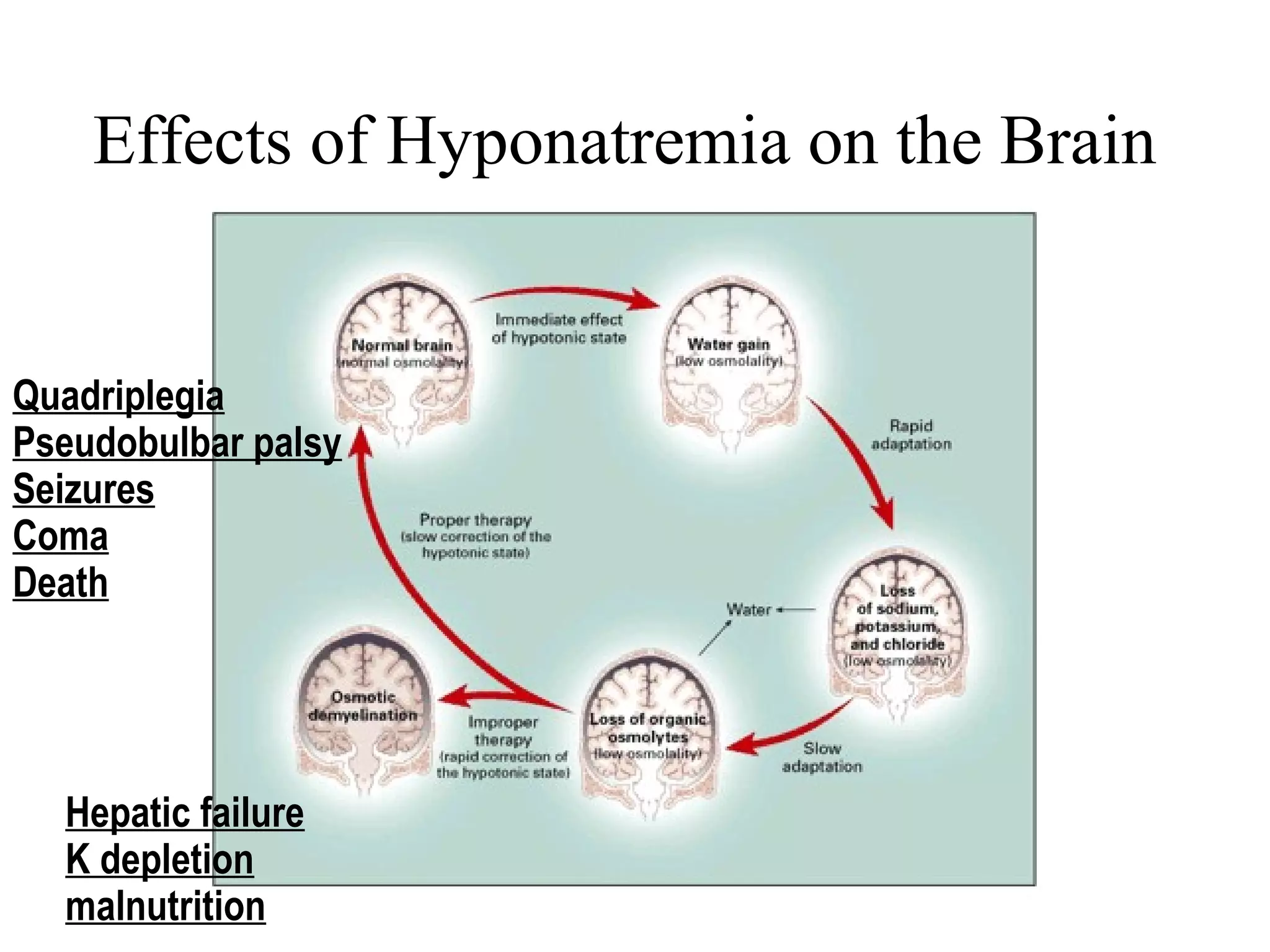
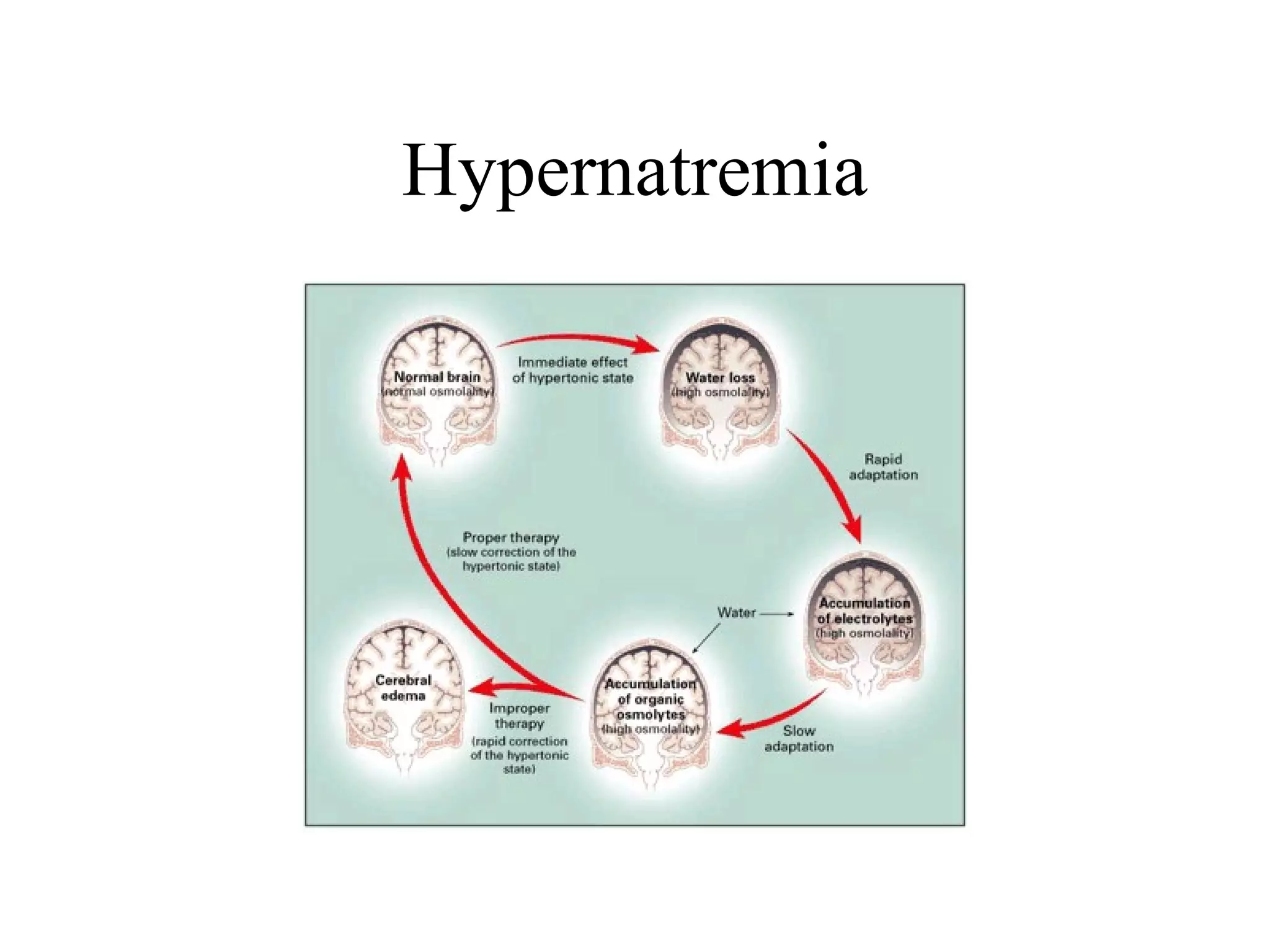
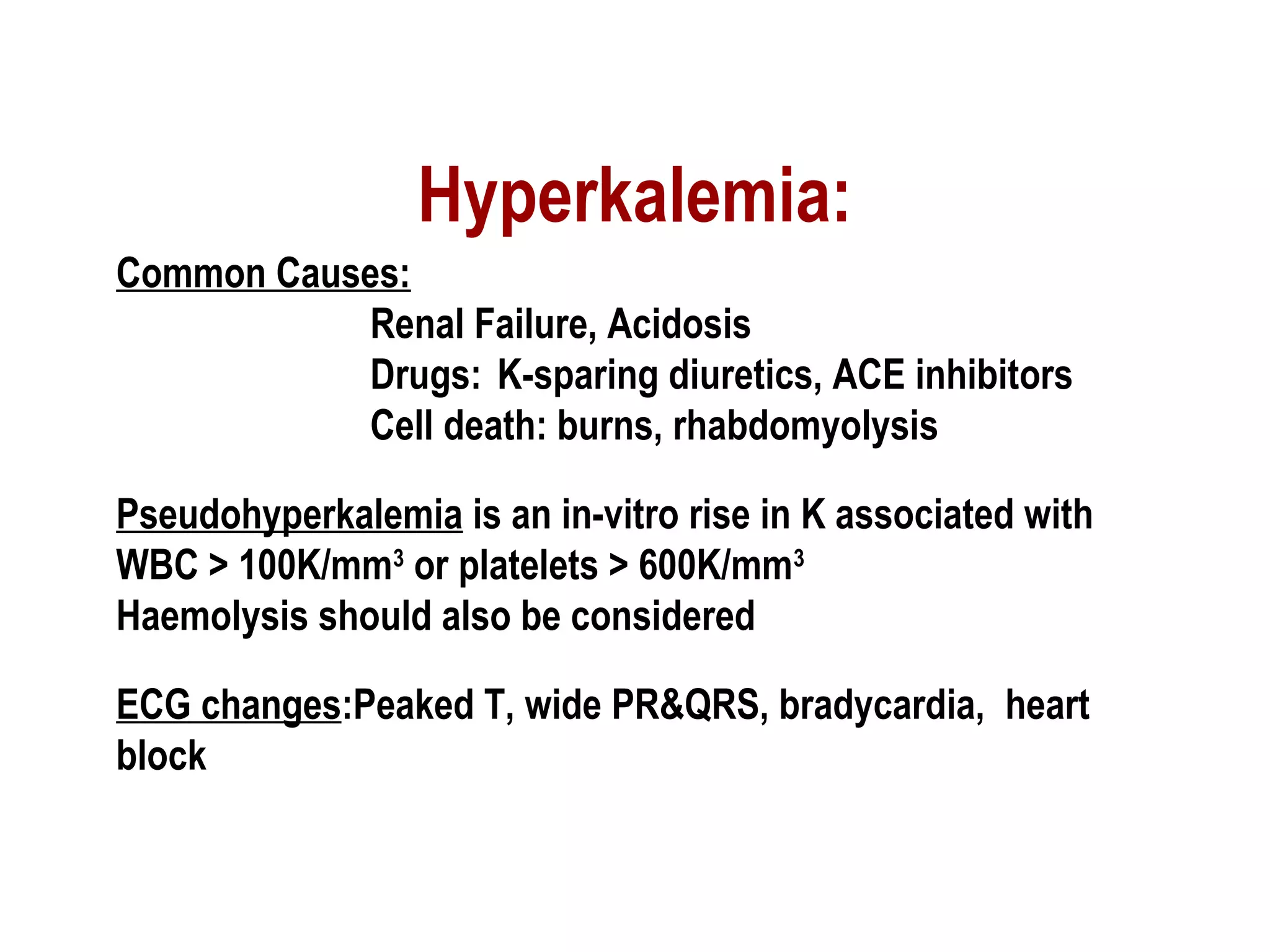
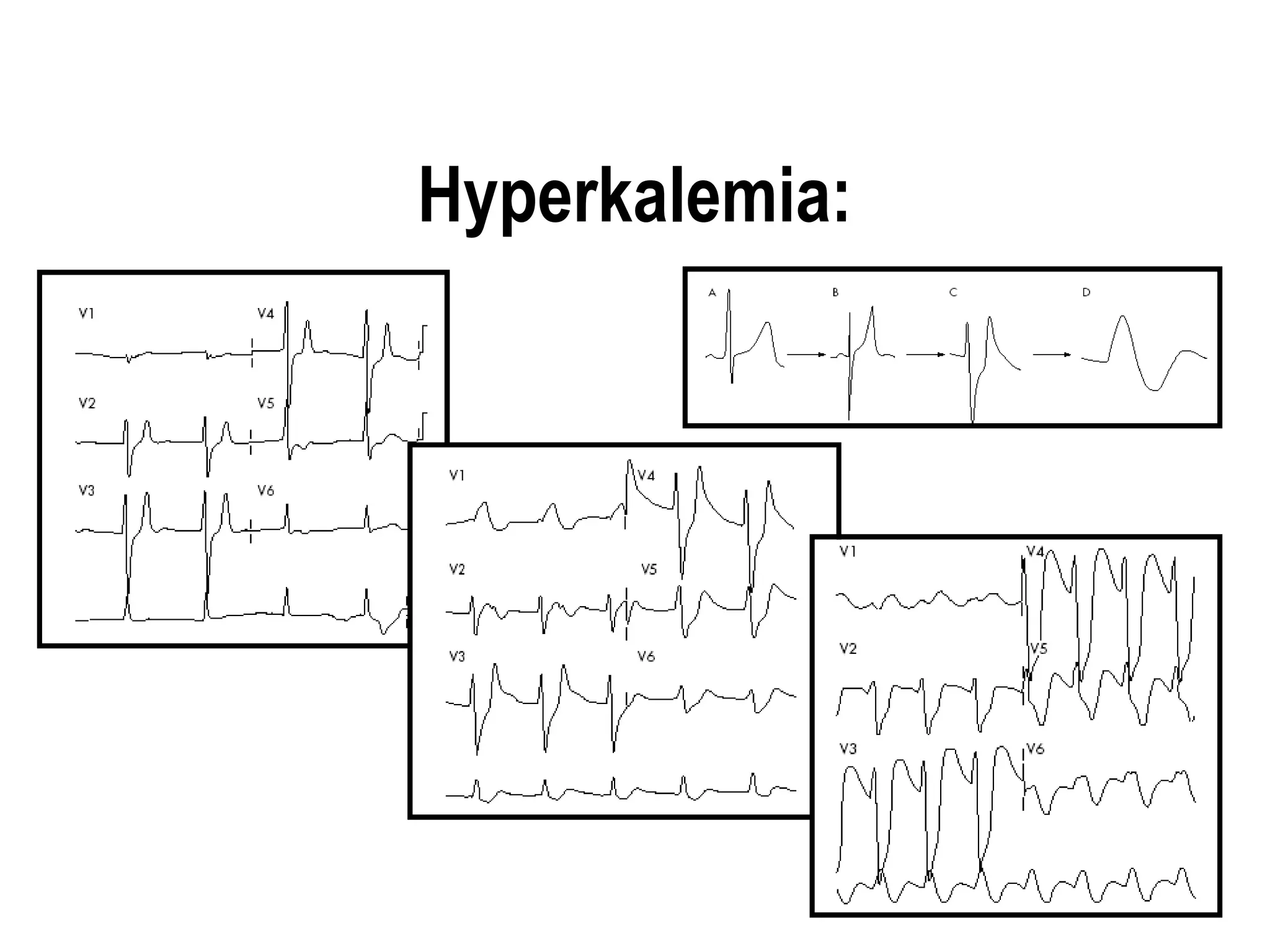

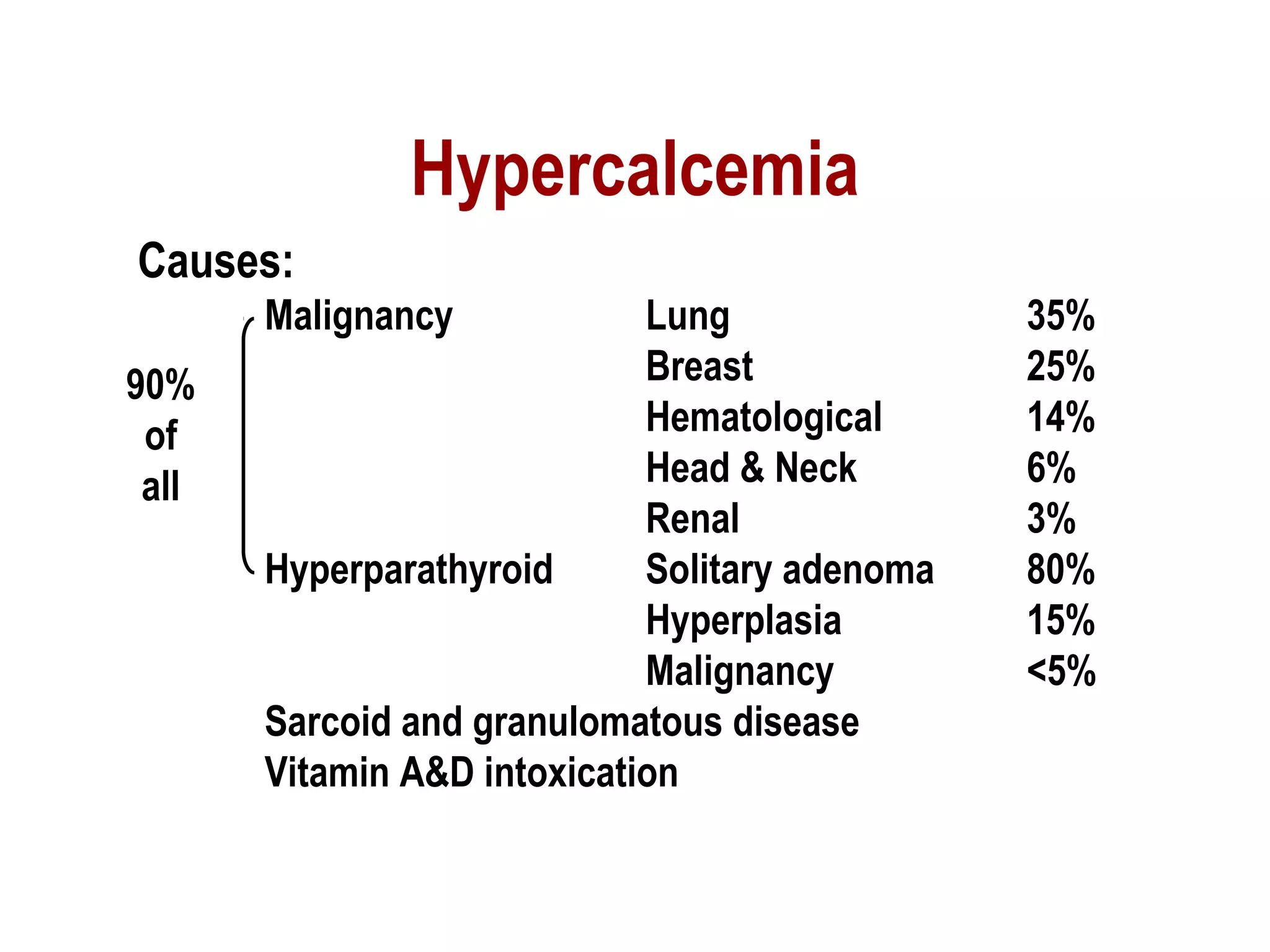



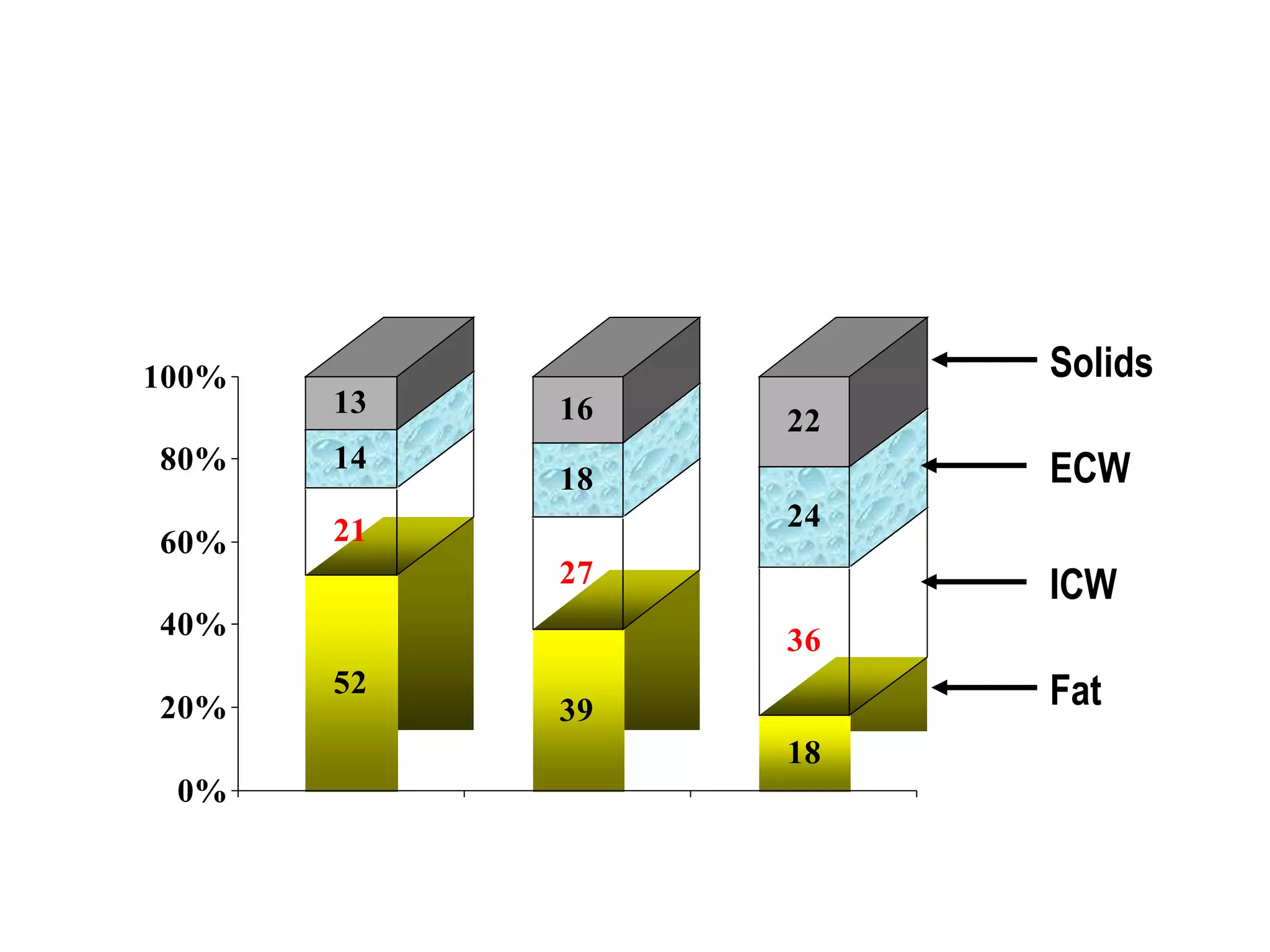
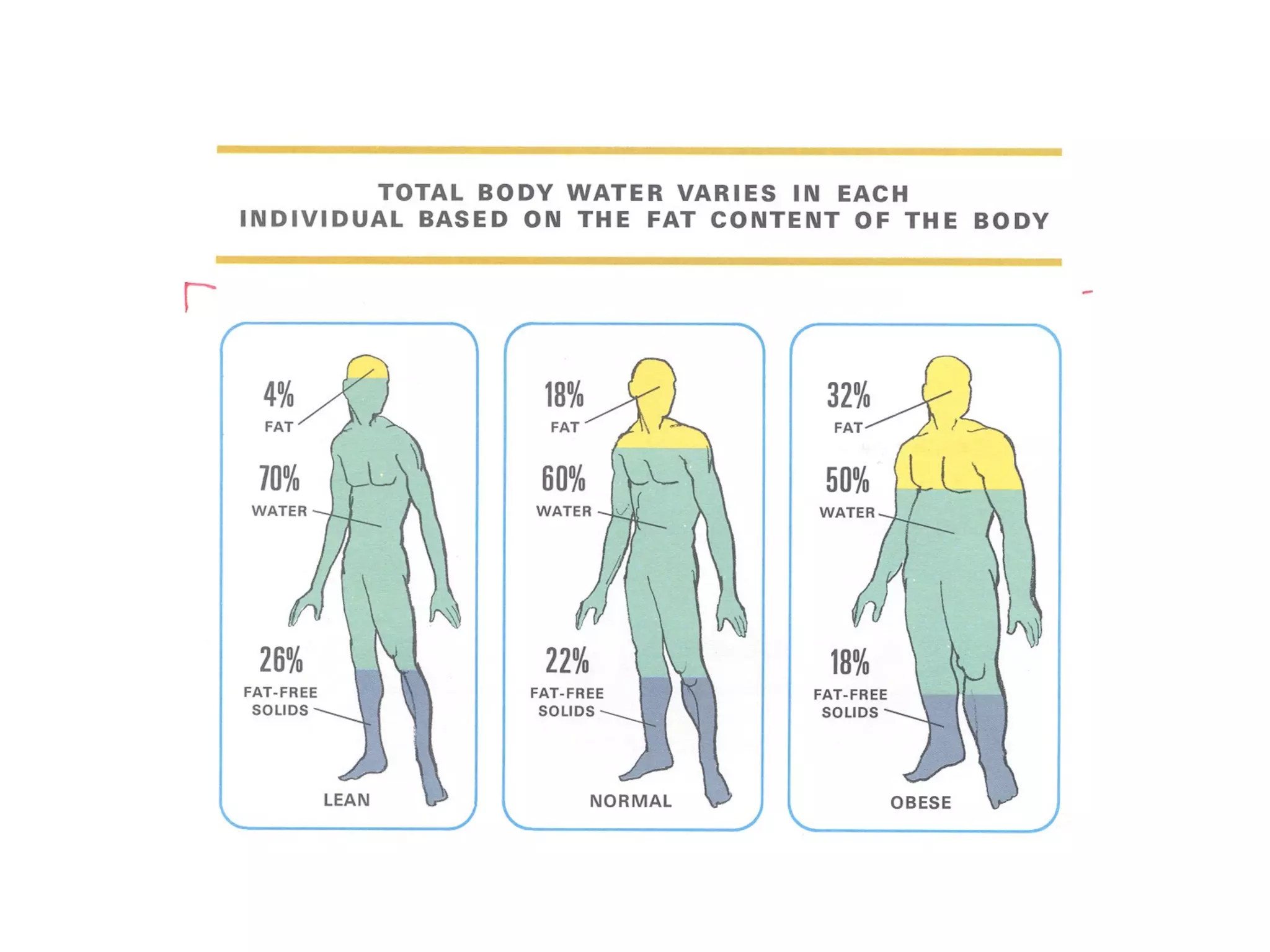
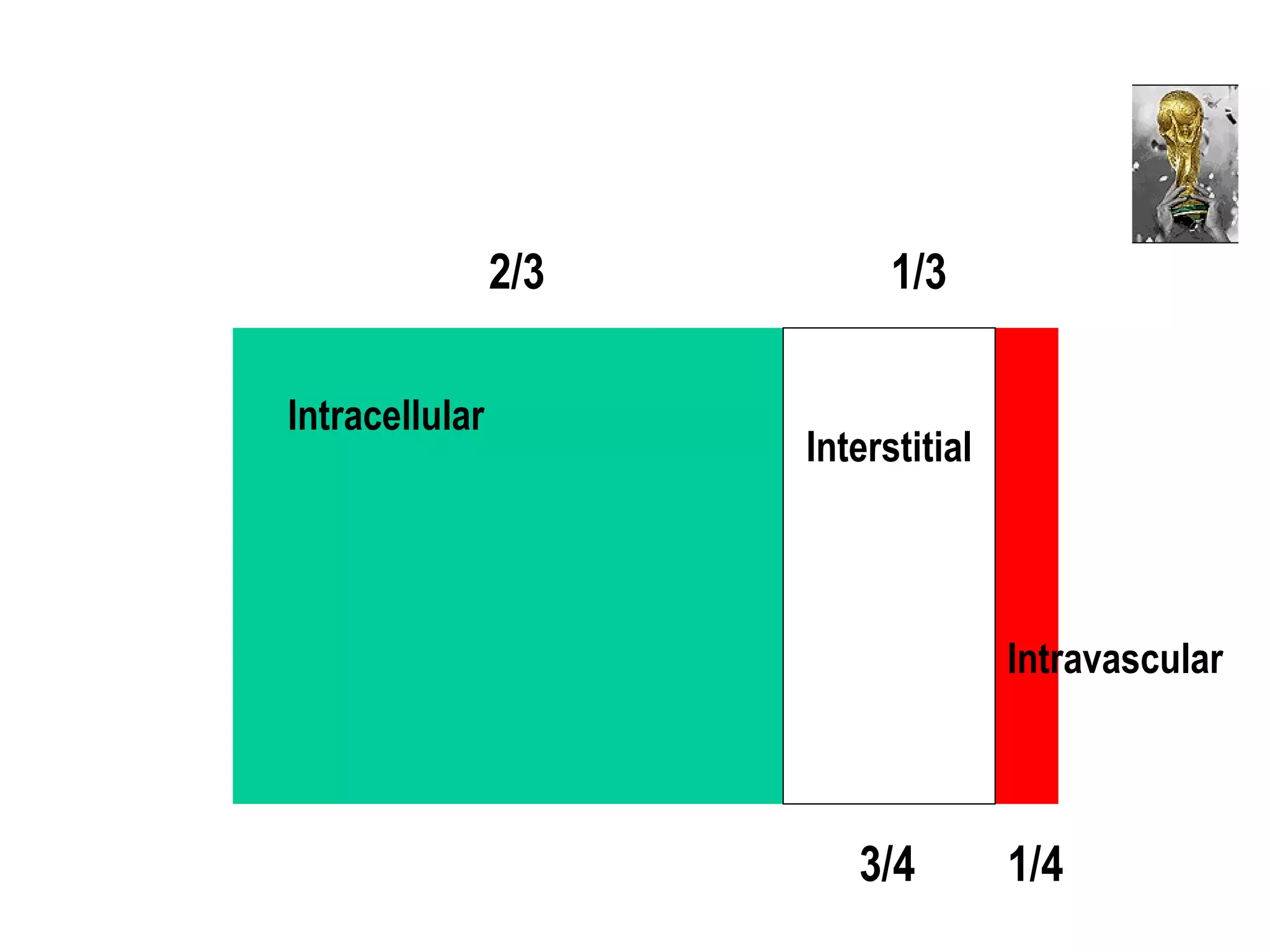
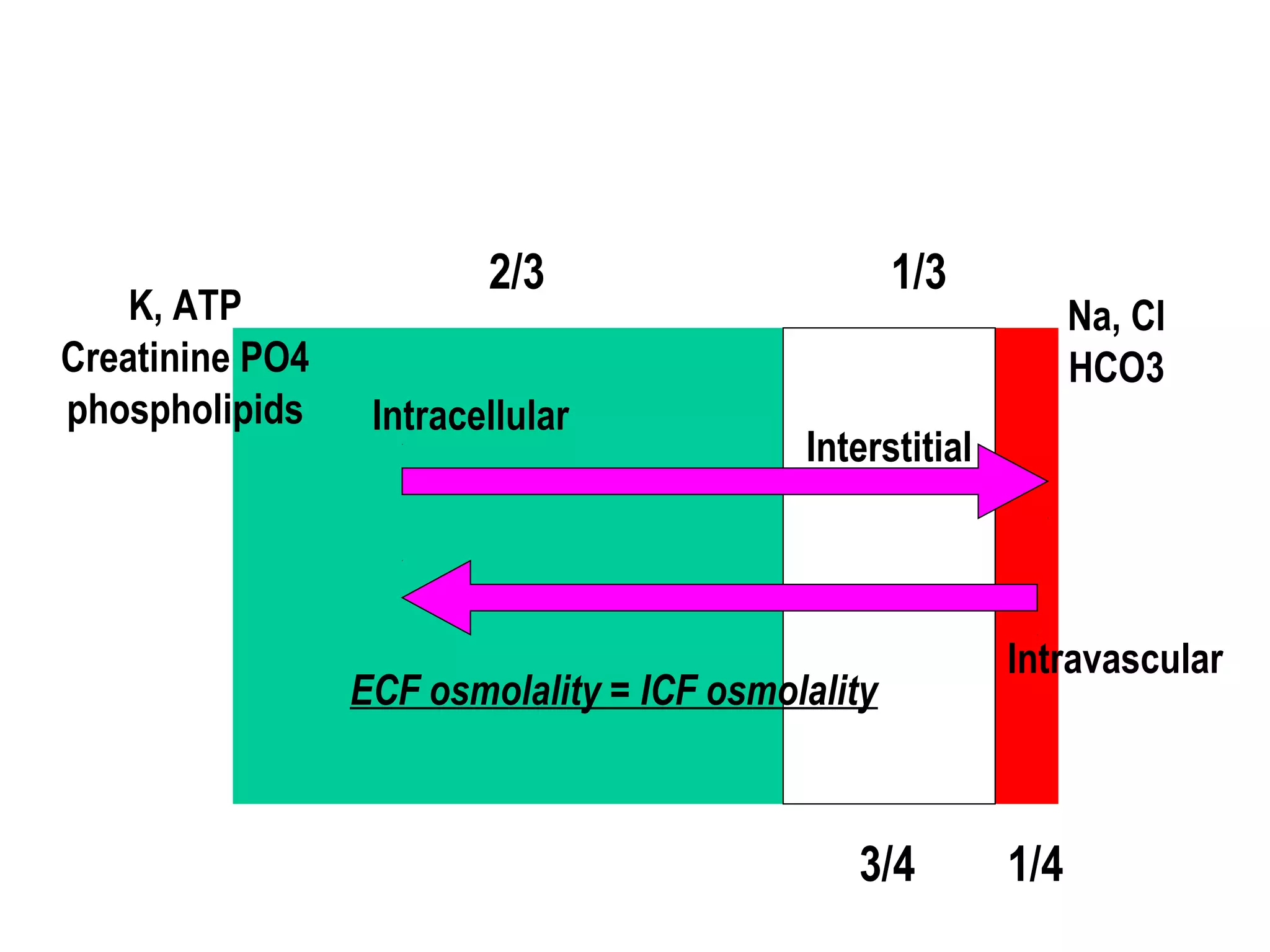
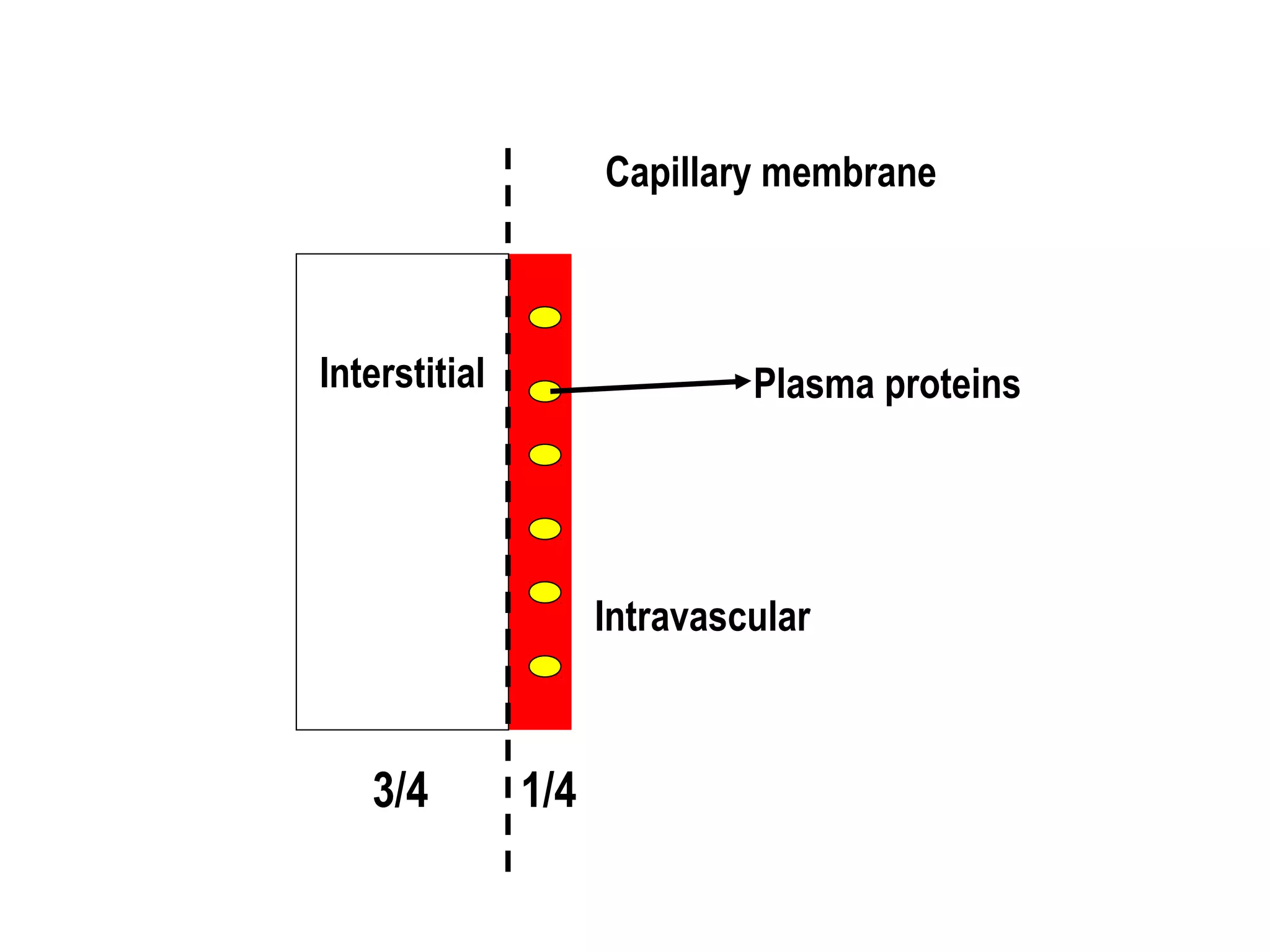
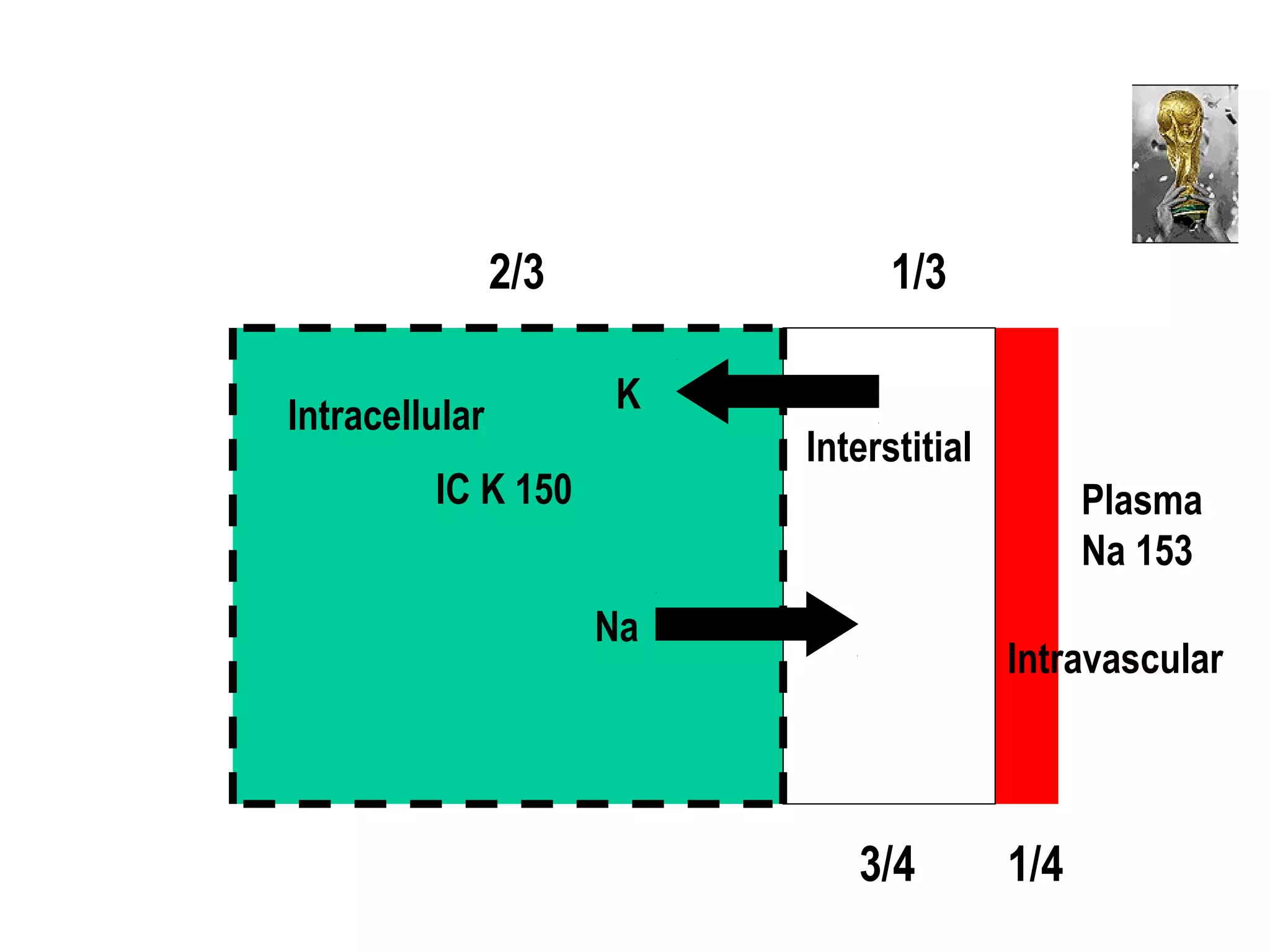
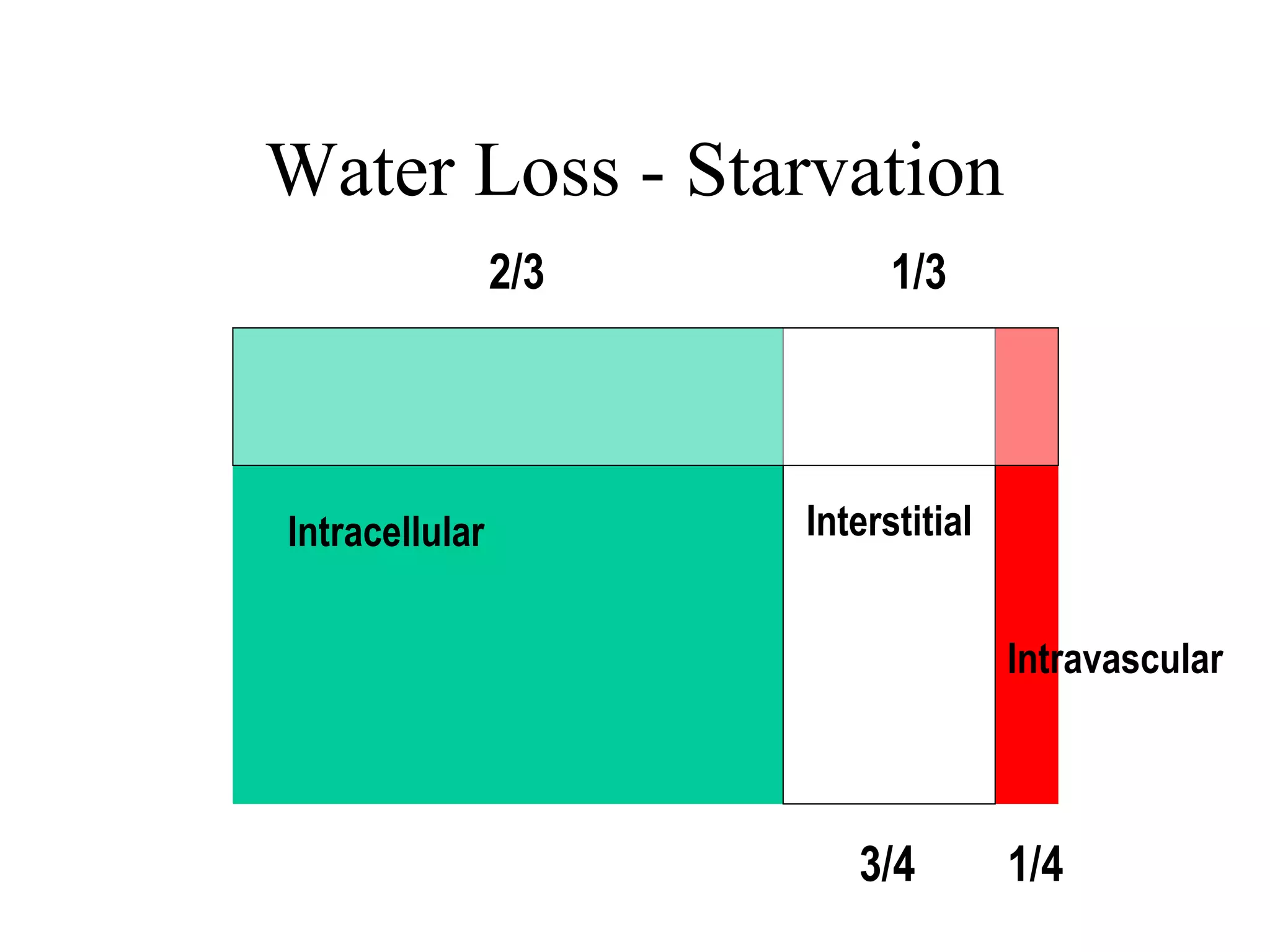
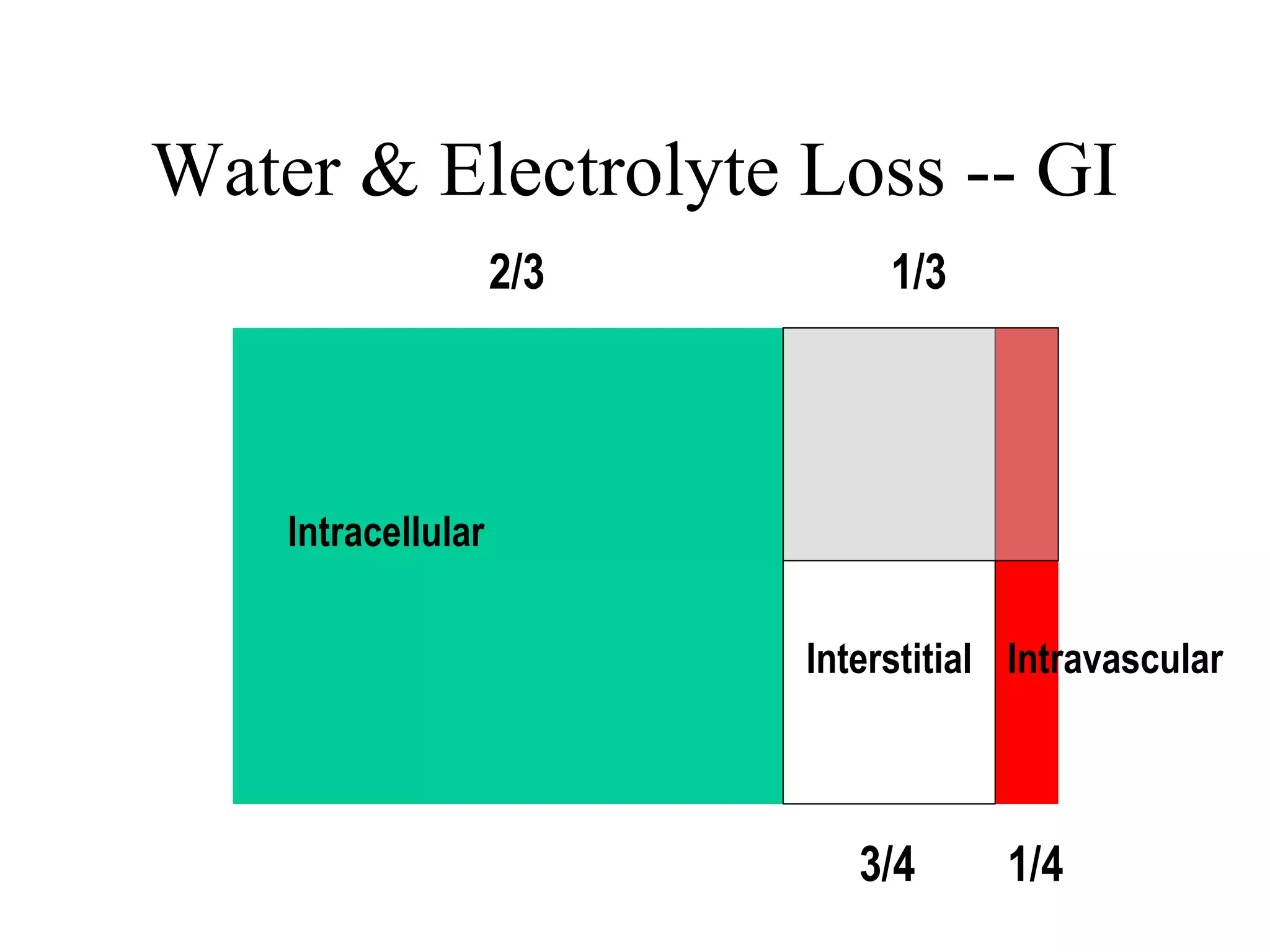
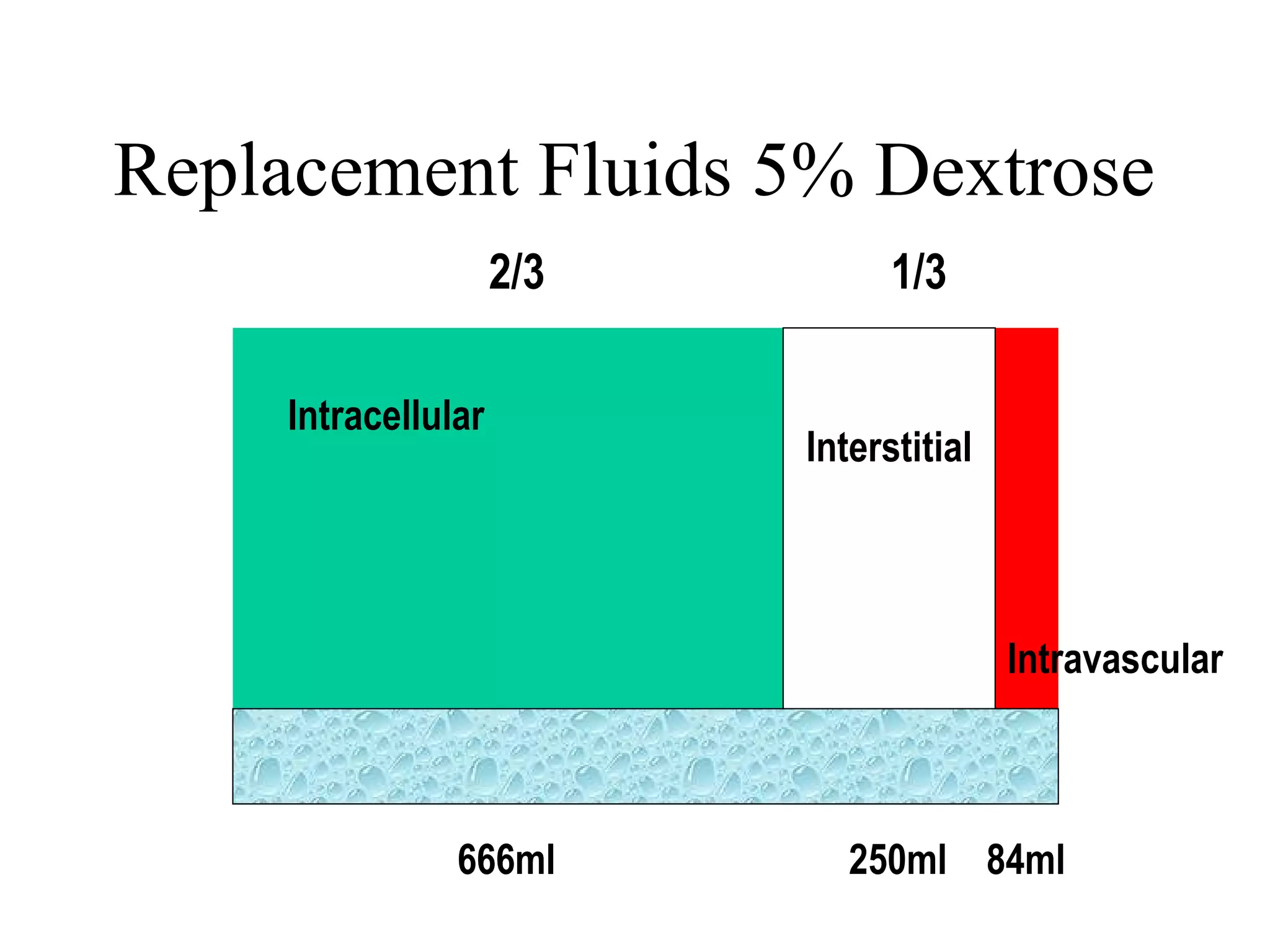
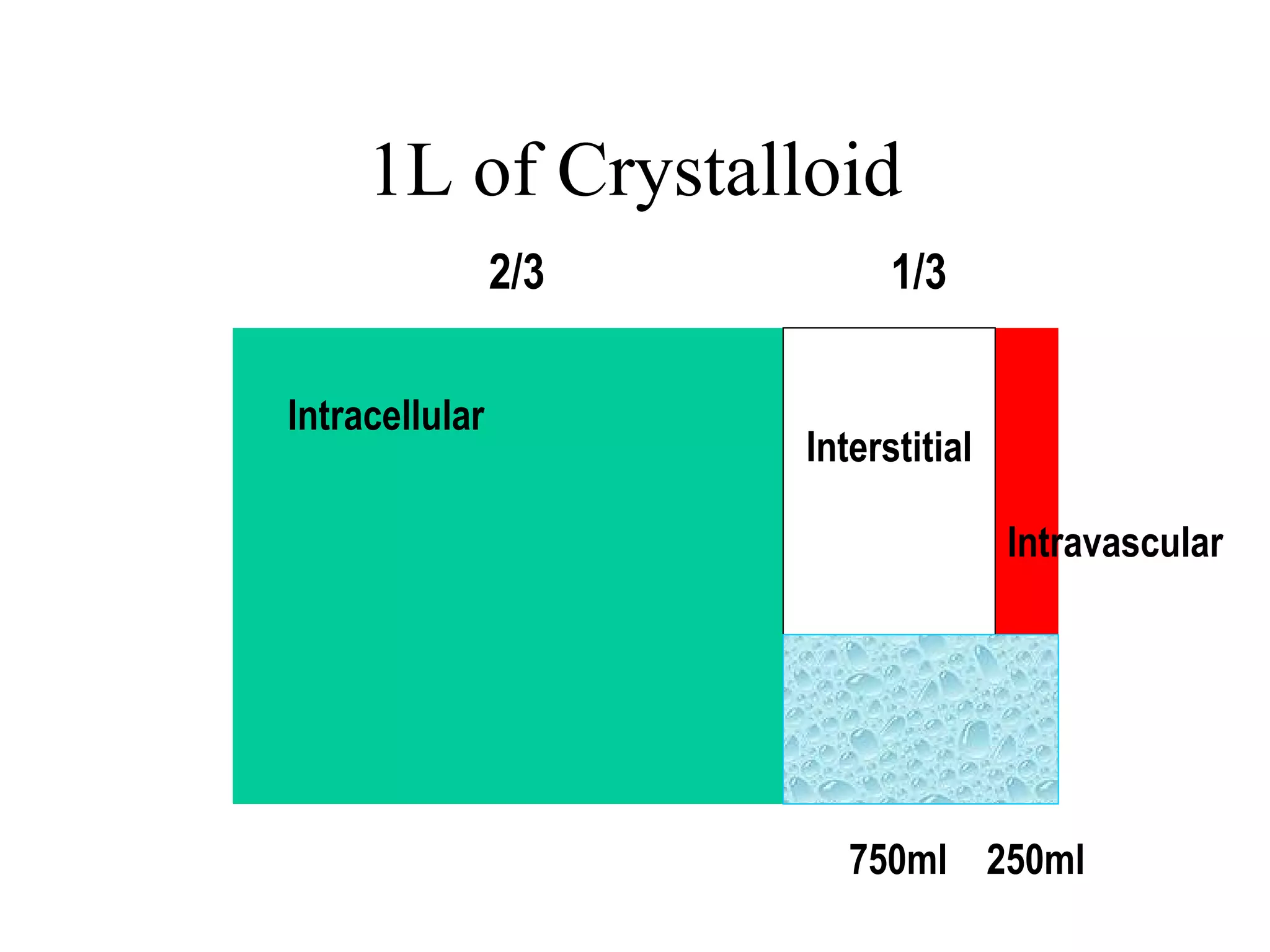
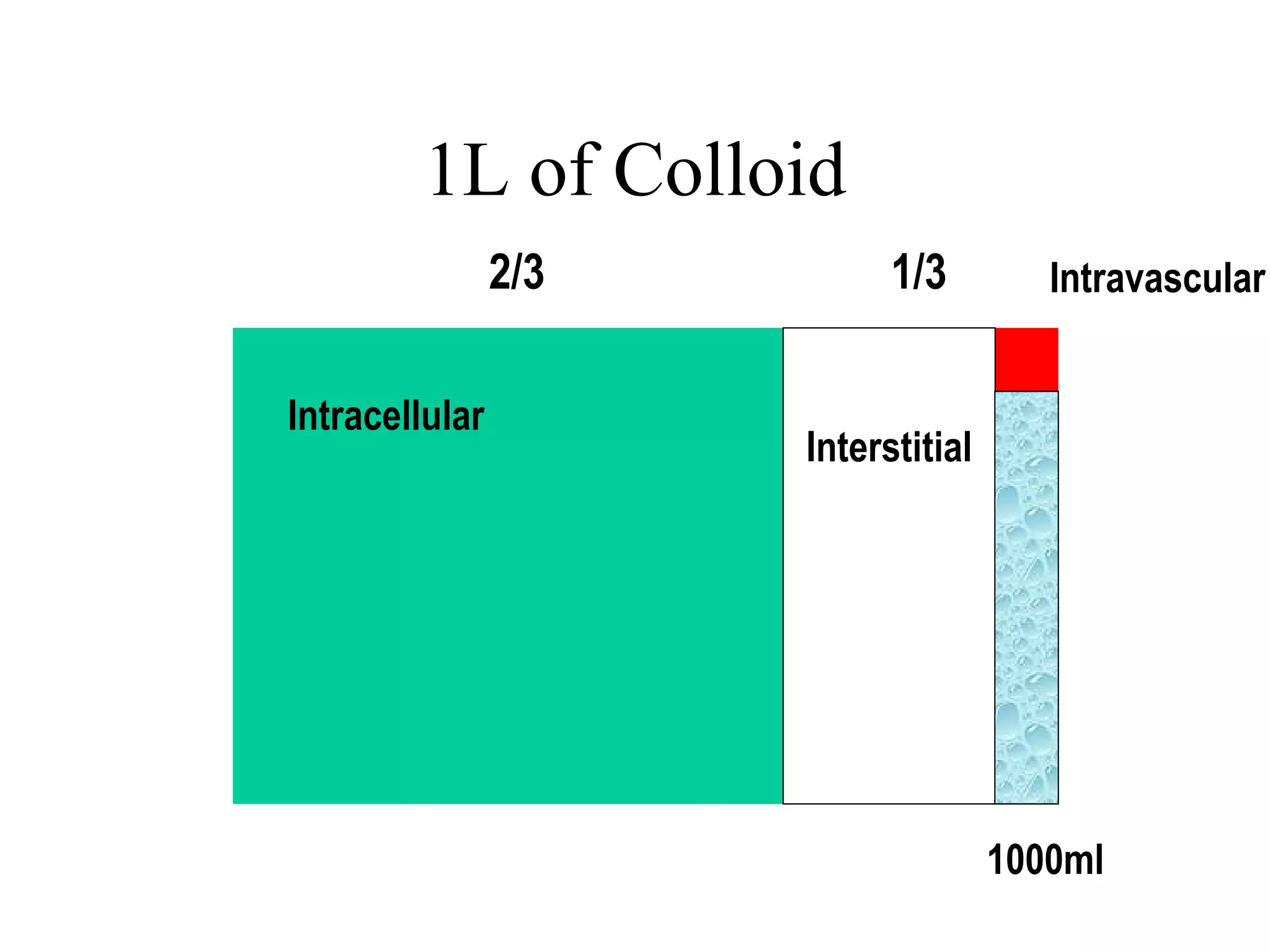
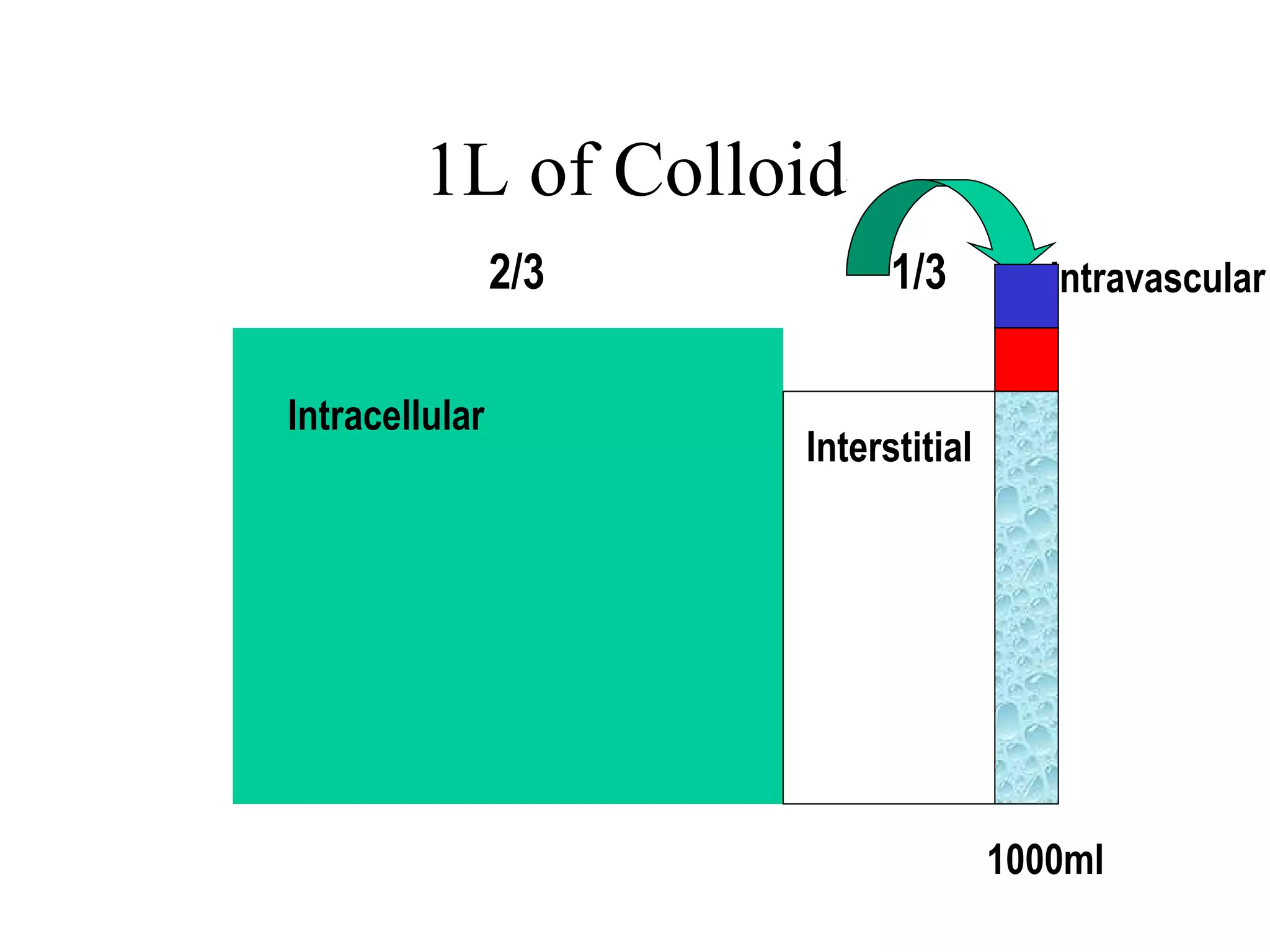
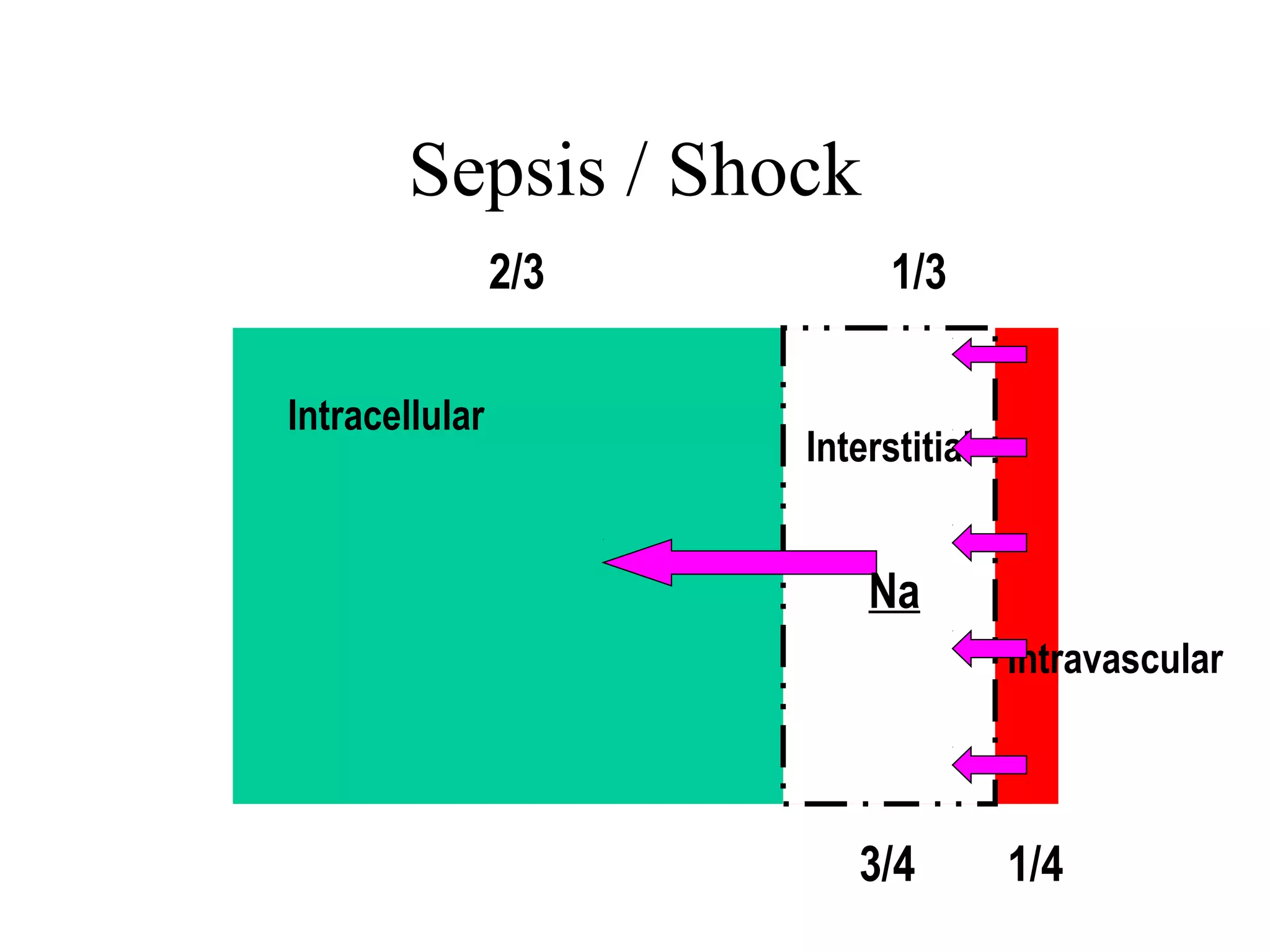
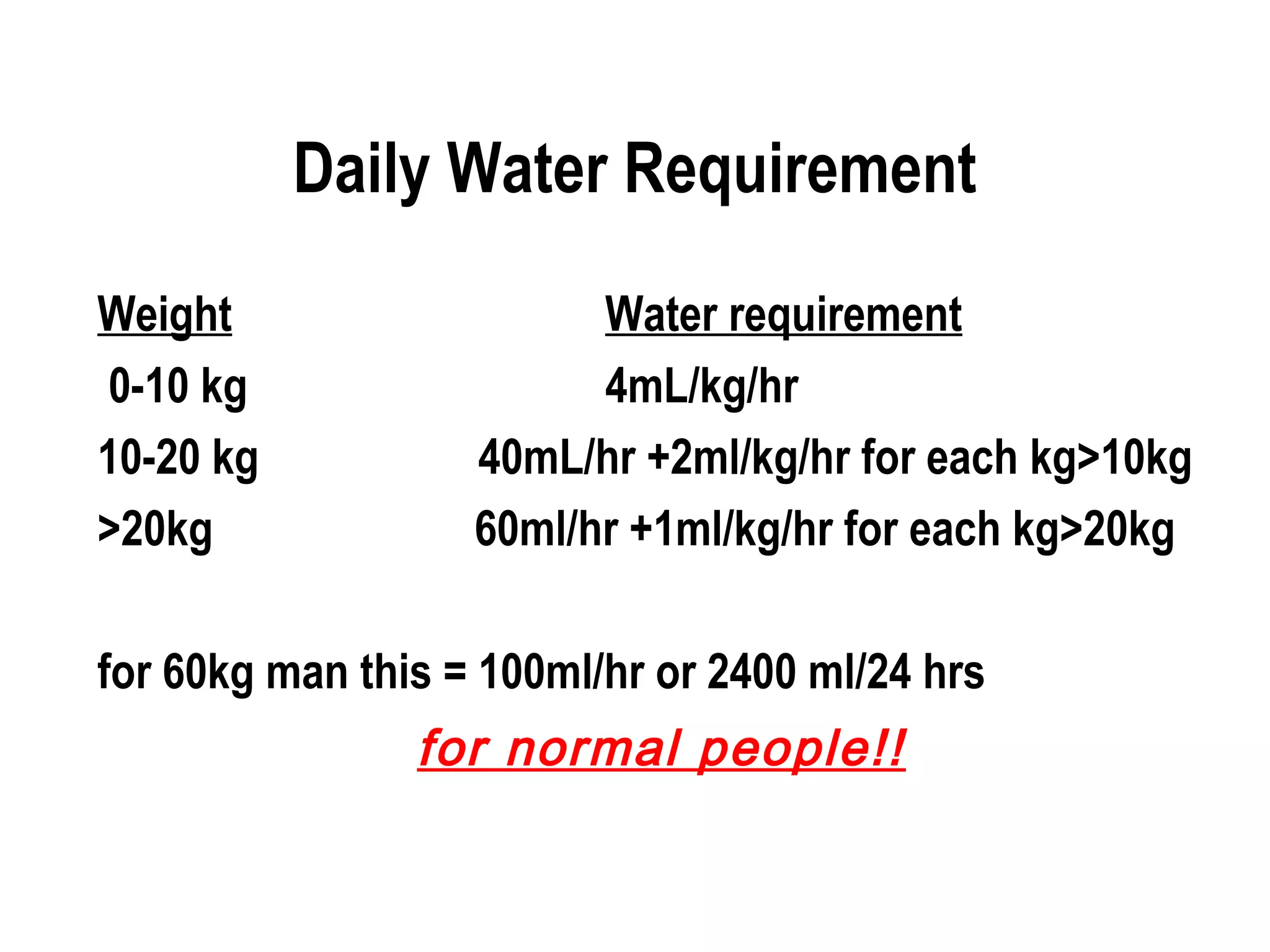
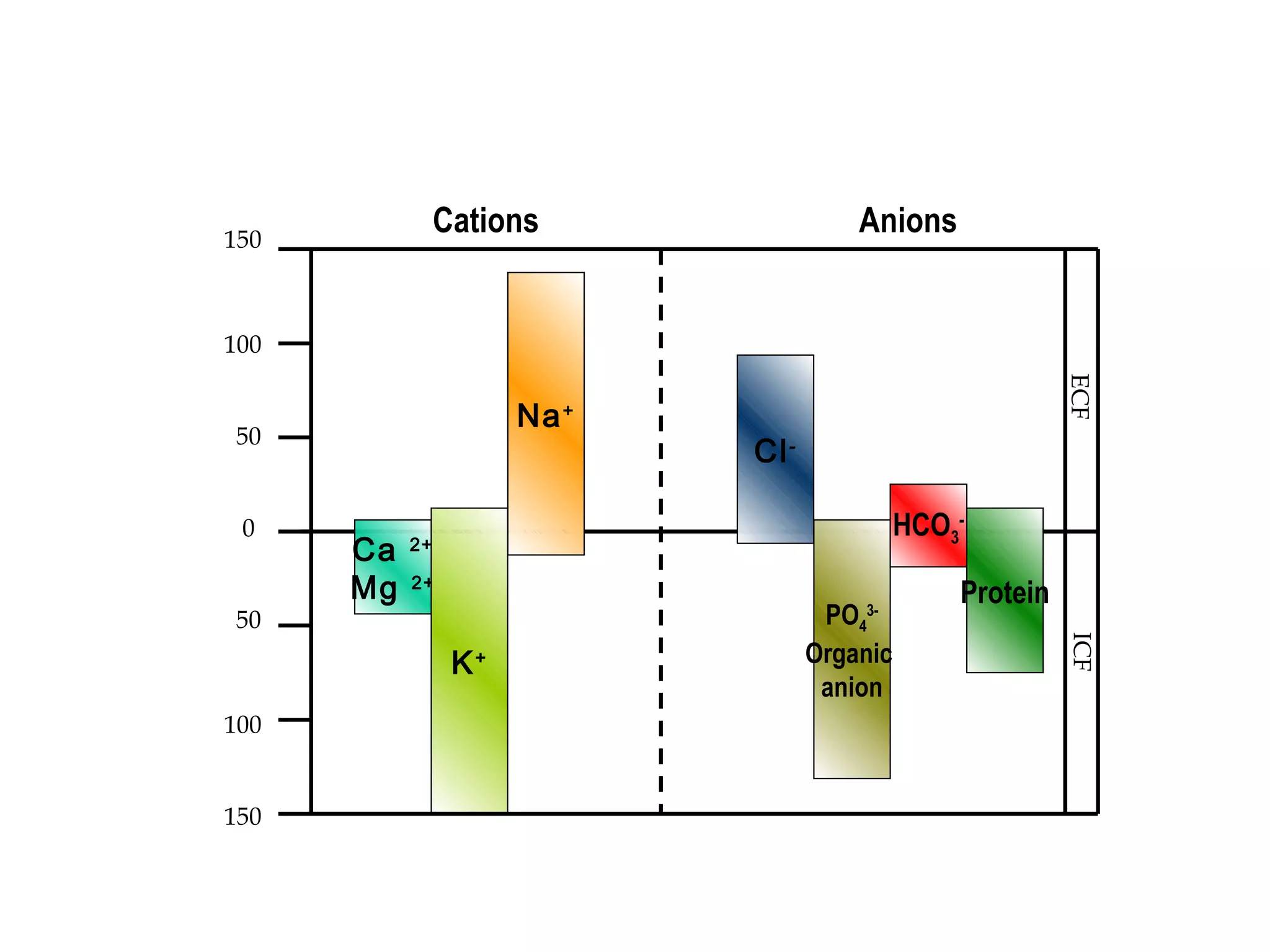
This document discusses fluid and electrolytes in the human body. It provides information on: - Water content and distribution in the body - Distribution of electrolytes like sodium, potassium, calcium, and magnesium between intracellular, interstitial, and intravascular fluid compartments - Daily water requirements - Causes, signs, and treatments of electrolyte abnormalities like hyponatremia, hypernatremia, hypokalemia, hyperkalemia, hypocalcemia, and hypercalcemia.










































































