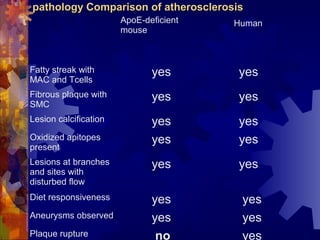
This document discusses animal models for studying vulnerable plaque and atherosclerosis. It describes how the chicken, pig, mouse, and rabbit models each have advantages and disadvantages for replicating different aspects of human disease. The mouse has been genetically modified to better model plaque development. No single animal model fully captures the human condition, but they provide insights into disease mechanisms. The document also notes that no current animal model replicates the plaque rupture seen in human heart attacks.





































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
