
More Related Content
Similar to 003 adult burns
Similar to 003 adult burns (20)
Recently uploaded
Recently uploaded (20)
003 adult burns
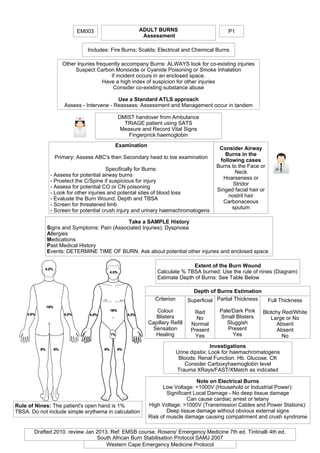
- 1. EM003 ADULT BURNS Assessment Includes: Fire Burns; Scalds; Electrical and Chemical Burns Take a SAMPLE History Signs and Symptoms: Pain (Associated Injuries); Dyspnoea Allergies Medications Past Medical History Events: DETERMINE TIME OF BURN. Ask about potential other injuries and enclosed space Extent of the Burn Wound Calculate % TBSA burned: Use the rule of nines (Diagram) Estimate Depth of Burns: See Table Below Consider Airway Burns in the following cases Burns to the Face or Neck Hoarseness or Stridor Singed facial hair or nostril hair Carbonaceous sputum Depth of Burns Estimation Criterion Colour Blisters Capillary Refill Sensation Healing Superficial Red No Normal Present Yes Partial Thickness Pale/Dark Pink Small Blisters Sluggish Present Yes Full Thickness Blotchy Red/White Large or No Absent Absent No Investigations Urine dipstix: Look for haemachromatogens Bloods: Renal Function. Hb. Glucose. CK Consider Carboxyhaemoglobin level Trauma XRays/FAST/XMatch as indicated Note on Electrical Burns Low Voltage: <1000V (Household or Industrial Power): Significant Local Damage - No deep tissue damage Can cause cardiac arrest or tetany High Voltage: >1000V (Transmission Cables and Power Stations): Deep tissue damage without obvious external signs Risk of muscle damage causing compatrment and crush syndrome Drafted 2010. review Jan 2013. Ref: EMSB course. Rosens' Emergency Medicine 7th ed. Tintinalli 4th ed. South African Burn Stabilisation Protocol SAMJ 2007 P1 Western Cape Emergency Medicine Protocol Other Injuries frequently accompany Burns: ALWAYS look for co-existing injuries Suspect Carbon Monoxide or Cyanide Poisoning or Smoke Inhalation if incident occurs in an enclosed space. Have a high index of suspicion for other injuries Consider co-existing substance abuse Use a Standard ATLS approach Assess - Intervene - Reassess: Assessment and Management occur in tandem DMIST handover from Ambulance TRIAGE patient using SATS Measure and Record Vital Signs Fingerprick haemoglobin Examination Primary: Assess ABC's then Secondary head to toe examination Specifically for Burns: - Assess for potential airway burns - Proetect the C/Spine if suspicious for injury - Assess for potential CO or CN poisoning - Look for other injuries and potental sites of blood loss - Evaluste the Burn Wound: Depth and TBSA - Screen for threatened limb - Screen for potential crush injury and urinary haemachromatogens Rule of Nines: The patient's open hand is 1% TBSA. Do not include simple erythema in calculation
- 2. ADULT BURNS Management EM003 Stabilise ABC's Manage the Burn Wound: Remove the source of heat Cool burns <3 hrs old - rinse with tepid tap water for minimum half hour Remove clothing/jewellery/rings Escharotomies for circumferential burns of the limbs or chest Apply burnshield (or clingfilm) once cooled for first 6 hrs - After 24 hrs use flamazine dressings Give TETANUS and Analgesia Indications for Intubation Airway Burns with predicted deterioration GCS < 8 or inability to maintain airway Not oxygenating Not ventilating Fluid Management If > 20 % TBSA: Insert 2 x large bore IV cannulas (Can be inserted through burned skin) Difficult IV acces: Femoral/Extrenal Jugular/ large bore CVP or IO lines. Cut-down. Insert Urinary Catheter A shocked patient needs to be resuscitated: Give crystalloid boluses (20ml/kg) until shock is reversed. If the patient is bleeding, blood transfusion is indicated Further fluid is given to replace losses occurring through burned skin This is given in addition to any resuscitation fluid needed PARKLANDS FORMULA Calculates the amount of fluid needed over the first 24 hours Calculated from the TIME OF THE BURN 4 ml/kg x Weight x % Body Surface Area Burned Give half over the first 8 hours Give the next half over the next 16 hours Add 10% TBSA if there are associated airway burns MONITOR RESPONSE: Reassess hourly Keep Urine Output > 0,5 ml/kg/hr Monitor HR; BP; ABG; Lactate IV Analgesia - Morphine Reconstitute 10mg in 10 ml water Loading dose: 0.1-0.15 mg/kg (Use less for elderly or frail) Then Bolus 0.05 mg/kg every 15 min Titrate to analgesic effect Beware of decreased BP and respiratory depression Chemical Burns Remove all Clothing Wash with copious amounts of tap water If eyes involved - Irrigate until ph is normal Electrical Burns Attach cardiac monitor May need extra IV fluid Monitor for crush and compartments syndromes 1. >10% BSA any burn thickness 2. Any full thickness burn 3. Electrical or Chemical burns 4. Inhalation burns 5. Hands,Feet,Perineum,Face,Joints 6. Circumferential burns 7. Associated major trauma 8. Extremes of age > 65 9. Severe co-existing medical condition Contact Tygerberg Burns Unit 021-938 84911 If they do not have a bed, refer to secondary level surgical service in your area No admission criteria Stable These patients can be seen and discharged from every level of care with the following Ensure tetanus given Provide analgesia Arrange follow-up for dressings To return earlier if any signs of infection P2 Drafted 2010. review Jan 2013. Ref: EMSB course. Rosens' Emergency Medicine 7th ed. Tintinalli 4th ed. South African Burn Stabilisation Protocol SAMJ 2007 Western Cape Emergency Medicine Protocol Attach Monitors - ECG, SpO2, BP cuff Insert Urinary Catheter and NGT. (Not if Base of Skull Facture) Disposition Discharge Admit - Level 3 Burns Centre