Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Retrograde Intramedullary Nail with Femoral Head Allograft for Large Deficit Tibiotalocalcaneal Arthrodesis: RAIN Database
Similar to Retrograde Intramedullary Nail with Femoral Head Allograft for Large Deficit Tibiotalocalcaneal Arthrodesis: RAIN Database (20)
More from skisnfeet
More from skisnfeet (7)
Retrograde Intramedullary Nail with Femoral Head Allograft for Large Deficit Tibiotalocalcaneal Arthrodesis: RAIN Database
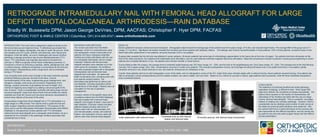
- 1. RETROGRADE INTRAMEDULLARY NAIL WITH FEMORAL HEAD ALLOGRAFT FOR LARGE DEFICIT TIBIOTALOCALCANEAL ARTHRODESIS—RAIN DATABASE Bradly W. Bussewitz DPM; Jason George DeVries, DPM, AACFAS; Christopher F. Hyer DPM, FACFAS ORTHOPEDIC FOOT & ANKLE CENTER | Columbus, OH | 614-895-8747 | www.orthofootankle.com INTRODUCTION: The lower limb is designed to adapt to terrain as the foot encounters ground reactive forces. To effectively accomplish this, the foot must be stable, plantigrade, and able to reach the ground. Ankle and subtalar joint (STJ) pain, arthritis, and deformity, both natural and iatrogenic, limits this ability. As one is challenged with severe hindfoot pathology a salvage procedure may involve tibiotalocalcaneal (TTC) fusion. TTC arthrodesis was originally described by Russotti and Johnson in 1988 to surgically correct these challenging scenarios (1). Correction is driven at achieving a painless, stable, plantigrade foot, with or without bracing. Additional complexity is encountered by the foot and ankle surgeon intraoperatively when a large bone void is presented during a TTC fusion. Loss of quality bone and/or loss of length in the lower extremity typically presents following avascular necrosis of the talus, Charcot neuroarthropathy of the ankle, longstanding gross malalignment, and iatrogenic changes, both acute and revisional. Regardless of the etiology, surgical correction must address the loss of height. One method of regaining bony height is by adding a structural graft at the time of fusion. There is considerable morbidity with taking large volume structural autograft. Large bone block frozen femoral heads are readily available and meet the volume and structural demands necessitated to restore bony defects at the level of the ankle. Incorporating a large bone block allograft into a TTC arthrodesis in a single stage is a difficult task. Few reports exist to guide the foot and ankle surgeon regarding outcome expectations. The purpose of this study was to use the Retrograde Arthrodesis Intramedullary Nail (RAIN) Database to retrospectively review patients with TTC arthrodesis utilizing femoral head allograft and a retrograde intramedullary rod as a treatment for the morbidity of the pathologic hindfoot associated with substantial loss of bone. MATERIALS AND METHODS: This review was taken from the RAIN Database, which is a comprehensive chart and radiographic review constructed of all patients who have undergone extended hindfoot and ankle arthrodesis with the use of a retrograde arthrodesis nail at a single institution. Patients with femoral head allograft utilization were selected out of the entire group for evaluation. All conditions that were surgically treated with a retrograde intramedullary nail and femoral head allograft were evaluated. All cases had failed conservative care, including some with joint sparing surgical options. The arthrodesis was performed to relieve pain and disability, including restoration and/or maintenance of limb length. Patients were all counseled on the risk of operative management. Inclusion criteria in this specific study were all patients entered into the RAIN Database that were treated with a femoral head allograft, and surgery at least 1 year prior to data collection. Exclusion criteria included patients treated primarily with forms of fixation other than an intramedullary nail, and included plates, screws, and external fixation, and restoration of bony voids with options other than femoral head allograft. RESULTS: Eleven patients fit inclusion criteria and were evaluated. Demographic data showed the average age of the patients was 54.6 years (range, 47 to 64), and included eight males. The average BMI of the group was 31.7 (range, 21.3 to 46.2). Significant risk factors revealed five smokers and three patients with diabetes mellitus. The etiology was Charcot neuroarthropathy in three patients, AVN in three patients, revisional fusion in two, failed total ankle replacement in two patients, and post-traumatic DJD in one patient. Surgical data revealed that the left side was affected in seven patients. All eleven patients had some type of orthobiologic augmentation to the fusion site at the time of surgery. Ten patients had bone stimulation at the time of the index procedure; four patients had implantable bone stimulation, and six used external combined magnetic field bone stimulation. Adjunctive procedures included a posterior muscle group lengthening in seven patients and complete talectomy in four. No patients had a tendon transfer or tarsal fusions. During followup after the surgery, the average time to protected weight bearing was 78.5 days (range, 42 – 204), and the time to full weightbearing was 124.8 days (range, 43 – 204). The average time to the final followup visit was 102.2 weeks (range, 28 to 180). Complications occurred in a total of six patients. This included postoperative incision and drainage including soft-tissue only in one patient and bone in one patient, partial hardware removal in one, stress fractures in two, and need for intravenous (IV) antibiotics in two. Overall, three patients went on to solid radiographic union of the ankle, and six radiographic unions of the STJ. Eight limbs were clinically stable with or without bracing. Seven patients required bracing. One patient was able to ambulate in shoes postoperatively and five walked unaided, two used a walker, and one other. Based on our criteria for success or failure, eight patients were successful, while the three transtibial amputations were considered failures. REFERENCES: Russotti GM, Johnson KA, Cass JR. Tibiotalocalcaneal arthrodesis for arthritis and deformity of the hind part of the foot. J Bone Joint Surg. 70A:1304-1307, 1988. CONCLUSION: The treatment of combined hindfoot and ankle pathology, regardless of etiology, is difficult to treat. When faced with large bony deficits, the complexity increases dramatically. The authors have reported on the results of intramedullary nail arthrodesis of the hindfoot and ankle with the use of a large volume, femoral head allograft. This is a powerful, one-stage method of treating very complex pathology. However, there is considerable risk as relatively small number of solid unions at the distal and proximal graft interfaces were observed. Still, the authors feel this is a useful technique as the success rate was reasonable for this difficult population, and the results can be useful to any foot and ankle surgeon faced with this difficult clinical presentation. Initial stabilization with external fixator Immediate post-op with internal fixation and femoral head 18 months post-op, with femoral head incorporated