
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Recurrent Metatarsal Synostosis Resection and Interposition with Human Allogenic Dermal Tissue Matrix
Similar to Recurrent Metatarsal Synostosis Resection and Interposition with Human Allogenic Dermal Tissue Matrix (20)
More from skisnfeet
More from skisnfeet (6)
Recurrent Metatarsal Synostosis Resection and Interposition with Human Allogenic Dermal Tissue Matrix
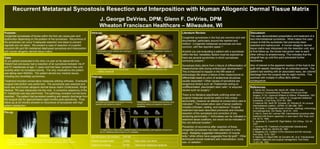
- 1. Recurrent Metatarsal Synostosis Resection and Interposition with Human Allogenic Dermal Tissue Matrix J. George DeVries, DPM; Glenn F. DeVries, DPM Wheaton Franciscan Healthcare – Milwaukee, WI Purpose: Congenital synostoses of bones within the foot can cause pain and dysfunction depending on the position of the synostosis. Recurrence of the synostosis can occur if adequate resection and steps to prevent regrowth are not taken. We present a case of resection of a painful recurrent 4th and 5th metatarsal diaphyseal synostosis and interposition with human allogenic dermal tissue matrix. Literature Review: Congenital synostoses in the foot are common and well documented, particularly around the rearfoot and midfoot. 1 Congenital metatarsal synostoses are less common, with few reported cases. 2,3 Anytime you are evaluating a patient with a synostosis within the foot, hereditary factors must be explored as there are several syndromes in which synostoses commonly present. 4 Synostosis likely stems from a failure of differentiation of mesenchymal cells during embryologic development. 2 This is theorized to happen in the fifth week or embryologic life where a failure of the mesenchyme to differentiate leads to union of anatomical structures usually seperated. 4 Other causes of synostosis are exogenous factors such as Thalidomide acting on undifferentiated, pleuripotent stem cells, 4 or acquired causes such as surgery. 5 There is no literature specifically outlining what non-surgical measures would be useful in this unique abnormality, however an attempt at conservative care is indicated. 3 The conservative care of tarsal coalitions includes orthoses, casting, and injections. 6 Surgical treatment has been described previously and includes resection of the synostosis and correction of any remaining abnormality. 2,3 Arthrodesis can be indicated in extensive tarsal coalitions, but would not be indicated in this non-articular location. 7 Prevention of recurrence after resection of these congenital synostoses has been attempted in a few ways. Badgeley suggested interposition of muscle belly, 8 while others have suggested free fat graft. 9 Other techniques include treatment with indomethacin, bone wax, or radiation. 1 Case : 35 y/o patient presented to the clinic c/o pain at his lateral left foot. Patient had previously had a resection of an synostosis between his 4 th and 5 th metatarsals at age 11 years and had been symptom free until recently when he increased activity. The only medications the patient was taking were NSAIDs. The patient denied any medical issues, including any hereditaty syndromes. Treatment included conservative measures utilizing orthoses. Eventually surgical intervention was performed. The synostosis was resected and bone wax and human allogenic dermal tissue matrix (GraftJacket, Wright Medical, TN) was interposed into the void. A corrective osteotomy of the 5 th metatarsal was also performed. The pathology revealed normal bone resected. The patient had persistent swelling and aseptic discharge from the surgical site for approximately eight months post-operatively. Final follow-up at 22 months showed no recurrence of synostosis with high patient satisfaction. Pre-op Post-op: Discussion : This case demonstrated presentation and treatment of a rare intermetatarsal synostosis. What makes this case unique is that the synostosis had previously been resected and hadrecurred. A human allogenic dermal tissue matrix was interposed into the resection void, and at final follow-up, the bones had grown near to each other without re-anastomosing This indicates that the allograft has up until this point prevented further recurrence. Also of interest is the apparent reaction of the host to the graft with aseptic discharge for an extended period. The patient had swelling with an associated waxy, tan colored discharge from the surgical site for eight months. This resolved with multiple in-office I&Ds without consequence. References: 1. Banks AS, Downey MS, Martin DE, Milller SJ (eds). McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery , 3 rd Ed. Lippincott Williams & Wilkins, Philadelphia, 1991. 2. Boccia JR, Dockery GL, LeBaron S. Congenital metatarsal synostosis. J Foot Surg. 23:41-45, 1984. 3. Kashuck KB, Hanft JR, Schabler JA, Wolosky B. An unusual intermetatarsal coalition. JAPMA. 81:384-388, 1991. 4. McCredie J. Congenital fusion of bones: radiology, embryology and pathogenesis. Clin Radiol. 26:47-51, 1975. 5. Atar D, Grant AD, Lehman WB. Intermetarsal synostosis after treatment with Ilizarov apparatus: a case report. Bull Hosp Joint Dis. 52:12, 1992. 6. Jaykamar S, Cowell HR. Rigid flatfoot. Clin Orthop. 122: 84, 1977. 7. Scranton PE. Treatment of symptomatic talocalcaneal coalition. JBJS-Am. 69:533-39, 1987. 8. Badgeley CE. Coalition of the calcaneus and the navicular. Arch Surg. 15:75, 1927. 9. Salamao O, Napoli MM, de Carvalho AE, et al. Talocalcaneal coalition: diagnosis and surgical management. Foot Ankle. 13:251-56, 1992. Pre-operative radiographs reveal large synostosis between 4 th and 5 th metatarsals across approximately 50% of the shaft length. Also there is significant lateral deviation of the 5 th metatarsal head AP Oblique Immediate post-operative radiographs showing resection and osteotomy fixation Radiographs at 12 months post-operative show osteotomy healing and apparent regrowth of synostosis CT taken at 22 months show excellent healing of the osteotomy, and regrowth of bone from the 5 th metatarsal without fusion to 4 th metatarsal Intra-op: Identification of the coalition and marking of resection margins Excision of coalition. Immediate mobility of 4 th and 5 th metatarsals Preparation of allograft for interposition between metatarsals Allograft fixated within resection void ACFAS Score (22 months) 68/100 Patient Questionnaire 28/50 Pain when non-shod Objective Findings 40/50 Abnormal metatarsal parabola