Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cannulated Screw Fixation of Jones 5th Metatarsal Fracture: Comparison of Titanium and Stainless Steel Screw Fixation
Similar to Cannulated Screw Fixation of Jones 5th Metatarsal Fracture: Comparison of Titanium and Stainless Steel Screw Fixation (20)
More from skisnfeet
More from skisnfeet (7)
Cannulated Screw Fixation of Jones 5th Metatarsal Fracture: Comparison of Titanium and Stainless Steel Screw Fixation
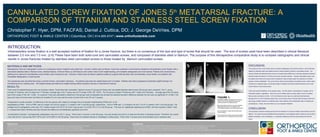
- 1. CANNULATED SCREW FIXATION OF JONES 5 th METATARSAL FRACTURE: A COMPARISON OF TITANIUM AND STAINLESS STEEL SCREW FIXATION Christopher F. Hyer, DPM, FACFAS; Daniel J. Cuttica, DO; J. George DeVries, DPM ORTHOPEDIC FOOT & ANKLE CENTER | Columbus, OH | 614-895-8747 | www.orthofootankle.com REFERENCES: 1.Dameron TB Jr. Fractures of the proximal fifth metatarsal: selecting the best treatment option. J Am Acad Orthop Surg 3:110-114, 1995. 2. Yue JJ, Marcus RE. The role of internal fixation in the treatment of Jones fractures in diabetics. Foot Ankle Int 17(9):559-562, 1996. 2. Glasgow MT, Naranja RJ, Glasgow SG, Torg JS. Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: the Jones fracture. Foot Ankle Int 17(8):449-457, 1996. 4. Larson CM, Almekinders LC, Taft TN, Garrett WE. Intramedullary screw fixation of Jones fractures: analysis of failure. Am J Sports Med 30(1):55-60, 2002. DISCUSSION: The purpose of the current study was to compare radiographic and clinical results in Jones fractures treated by stainless steel cannulated screws to those treated by titanium cannulated screws. Our results indicate that although there may be an experimental difference in bending resistance between stainless steel and titanium (7,8) this may not be clinically relevant. Though cannulated screws may be weaker than solid core screws when compared in load to failure tests, the relevance to clinical practice remains debatable. This current study clearly demonstrates cannulated screws, either made of titanium or stainless steel, are strong enough to stabilize and heal troubled fractures such as the Jones fracture in the clinical arena. There are several limitations to the present study. First the study is retrospective in design, and is inherently limited in application. Next, the use of multiple sizes of screws adds a level of variation that we were not able to control. A 5.5 mm titanium screw may very well be biomechanically stronger than a 4.0 mm stainless steel screw, but we have shown clinically that all screws within this size range, whether titanium or stainless steel, were effective with comparable rates of healing and complications. Finally, the short follow-up is an important limitation. CONCLUSION: The physician’s decision-making process for the selection of a screw to fixate Jones fractures can be difficult. Our study has demonstrated that the decision to use stainless steel or titanium can be left to patient constraints, such as allergies, or physician preference without compromising the clinical result. INTRODUCTION: Intramedullary screw fixation is a well accepted method of fixation for a Jones fracture, but there is no consensus of the size and type of screw that should be used. The size of screws used have been described in clinical literature between 3.5 mm and 7.0 mm. (2-6) These have been both solid-core and cannulated screws, and composed of stainless steel or titanium. The purpose of this retrospective comparative study is to compare radiographic and clinical results in Jones fractures treated by stainless steel cannulated screws to those treated by titanium cannulated screws. MATERIALS AND METHODS: Retrospective chart and radiographic review of a consecutive series of patients was performed . Inclusion criteria were as follows: must have sustained a Jones fracture treated by intramedullary screw fixation with a cannulated stainless steel or titanium screw, skeletal maturity, minimum follow-up until fracture union and/or return to full weight bearing, and complete radiographic and chart records. Patients who received bone grafting as an adjunct to intramedullary screw fixation were included as well. Exclusion criteria were as follows: patients treated by surgical methods other than intramedullary screw fixation, and patients with incomplete radiographic or chart records. The procedures were all performed using a minimal incision, cannulated technique. All patients were kept non-weight bearing for 4-6 weeks. Patients were then progressed to protected weight bearing in an immobilizing boot or walking case. Full weight bearing was defined as weight bearing without protective devices or restrictions of activity. RESULTS: There were 53 patients/fractures who met inclusion criteria. Those fixed with cannulated titanium screws (Ti group) and those with cannulated stainless steel screws (SS group) were compared. The Ti group included 37 fractures, with 20 males and 17 females. Average age in the Ti group was 43.75 (range 16-80, SD: 16.56). The SS group included 16 fractures with 7 males and 9 females. Average age of the SS group was 43.93 (range 27-69, SD: 13.96). An unpaired T test was calculated to determine if the groups were comparable and showed the standard deviation difference between the two was not significant (P =0.483). The types and sizes of screws were recorded and revealed 5.0 mm size was the most common both in the SS and Ti groups. Postoperative results revealed no difference in the two groups with respect to average time to protected weightbearing (PWB) and to full weightbearing (FWB). Time to PWB was 6.3 (range 4-9) and 6.5 (range 4-11) weeks in the Ti and SS groups, respectively. Time to FWB was 11.5 (range 6-19) and 11.6 (8-17) weeks in the Ti and SS groups. The average time to radiographic union was 12.01 weeks (range 4-28, SD 5.10) in the Ti group and 13.4 (8-28, SD 5.71) in the SS group. This was not statistically significant (p=0.569) with the unpaired 2-tailed T-test. A nonparametric Mann-Whitney test also showed this difference not statistically significant (p=0.327). Complications included 1 asymptomatic radiographic nonunion in the Ti group. There were 2 nonunion in the SS group, one was revised and went on to heal and the other is awaiting revision. Therefore, the overall union rate for the Ti group was 36/37 (97%) and 14/16 (88%) in the SS group. There were no hardware failures or breakages in either group. Three of the Ti screws were removed later due to hardware pain. REFERENCES: 1.Dameron TB Jr. Fractures of the proximal fifth metatarsal: selecting the best treatment option. J Am Acad Orthop Surg 3:110-114, 1995. 2. Yue JJ, Marcus RE. The role of internal fixation in the treatment of Jones fractures in diabetics. Foot Ankle Int 17(9):559-562, 1996. 2. Glasgow MT, Naranja RJ, Glasgow SG, Torg JS. Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: the Jones fracture. Foot Ankle Int 17(8):449-457, 1996. 4. Larson CM, Almekinders LC, Taft TN, Garrett WE. Intramedullary screw fixation of Jones fractures: analysis of failure. Am J Sports Med 30(1):55-60, 2002. A B D C FIGURE 1: A) Medial oblique radiograph demonstrating Classic Jones’ 5th metatarsal base fracture extending toward 4th metatarsal base. B) Intraoperative fluoroscan view demonstrating appropriate placement of cannulated screw intramedullary guidewire and drilling past fracture. C) Post-operative 4 weeks demonstrating early fracture healing. D) Post-operative 8 weeks demonstrating healed Jones fracture with intramedullary screw fixation.