The document discusses the meticulous techniques and considerations involved in thyroidectomy, emphasizing the importance of preserving the recurrent laryngeal nerve and parathyroid glands during surgery. It outlines the surgical anatomy, preparation, operative procedure, types of thyroidectomy, and complications, while also highlighting historical contributions to the surgical field. Additionally, it includes detailed descriptions of relevant anatomical triangles, patient preparation strategies, and the significance of various anatomical structures related to thyroid surgery.
![THYROIDECTOMY
“Arenditionforpreservation”
DR. SIDDHARTH JINDAL
PG-3RD YEAR [SU-1]
DEPARTMENT OF SURGERY
P.D.U. GOVT. MEDICAL COLLEGE, RAJKOT
30-09-2021
1](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-1-320.jpg)



![VASCULAR SUPPLY
ARTERIAL
1. Superior thyroid artery
2. Inferior thyroid artery
3. Thyroid ima artery [3-10%]
4. Accessory thyroid arteries
[arise from tracheal & esophageal
arteries]
VENOUS
Superior thyroid vein
Middle thyroid vein [LIGATED FIRST, IF + ]
Inferior thyroid vein
[fuse-thyroidea ima—Lt. BCV]
Kocher's’ 4th thyroid vein – occasionally b/w
middle and inferior thyroid veins, joins
IJV/MTV/ITV
ANTERIOR JUGULAR VEINS: descends vertically in
sup. Fascia, at 2.5cm above sternum , pierces
deep fascia to enter suprasternal space.
Its not related to venous drainage of the gland.
30-09-2021
7](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-7-320.jpg)









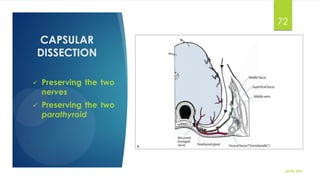
![TUBERCLE OF ZUCKERKANDL [Misc.]
TZ is postero-lateral projection from the thyroid lobe resulting at a point where lateral and the
medial components fuse.
Applied importance:
1. Grade 3 TZ: significant pressure symptoms, persistent after subtotal thyroidectomy
2. Intimately assoc. with RLN & Superior parathyroid. Enlargement occurs lateral to RLN—
The nerve appears to pass into a cleft medial to the enlarged tubercle.
3. Elevation of TZ: safe dissection; RLN passes medially through tunnel
4. The widened pre-vertebral space on X-ray of neck: (?) enlarged TZ [grade 2/3]
30-09-2021
18](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-18-320.jpg)



![BEAHR’S TRIANGLE
[RIDDLE’S]
USED TO IDENTIFY RLN CLOSE TO TEG
BOUNDARIES:
RLN [LOWER ARM]
INFERIOR THYROID ARTERY [SUPERIOR]
COMMON CAROTID ARTERY [BASE]
30-09-2021
22](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-22-320.jpg)




![JOLL’S TRIANGLE
[STERNOTHYROLARYNGEAL
TRIANGLE]
FOR IDENTIFICATION OF ESLN [LIES WITHIN]
BOUNDARIES:
FLOOR: CRICOTHYROID
SUPERIORLY: STRAP MUSCLES
LAT BORDER: SUP THYR. VESSELS & UPPER
POLE OF THYROID
30-09-2021
27](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-27-320.jpg)


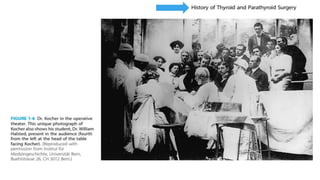
![Down the memory lane…
1912: KOCHER first thyroid surgery
Billroth, Kocher, Joll , Lahey and Galen: importance of laryngeal nerve preservation in thyroid
surgeries.
Illustration & description of nerves: Leonardo Di Vinci and Vesalius
20th century: Russian: Alexander Borbov: routine visual identification of nerves
George Crile: region of RLN , “no man’s land”
1935: Amelia Galli-Curci, famous opera singer [soprano], underwent a disastrous thyroid surgery,
EBSLN damaged.
Indian contribution: Sushruta [6th century B.C.] First to describe injury to neck at angle of jaw
voice hoarseness [? blood vessels]
Rufus and Ephesus: hoarseness was due to nerve injury and not vascular injury
30-09-2021
31](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-31-320.jpg)







![WORKUP
1. DL/IDL: VC check
2. CECT/MRI/intra-luminal imaging: potentially more advanced and regional disease
3. XRC [PA]- Retrosternal goiter
4. Decrease vascularity and risk of thyroid storm: anti-thyroid medications, beta blockers, lugol’s iodine [SSKI]
5. Rx of Beta-Blockers: continued for 7-10 days post-op because of longer t ½ of T4
6. MTC: r/o Phaeochromocytoma and MEN syndromes
7. Serum Calcium & PTH assay
8. In c/o thyroidectomy for solitary thyroid nodule, workup
TFT- serum TSH [higher TSH is an independent risk factor for malignancy]
USG, Radionuclide scintigraphy
FNAC
Thyroid suppression therapy 30-09-2021
41](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-41-320.jpg)










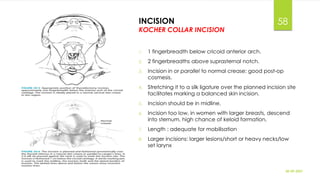



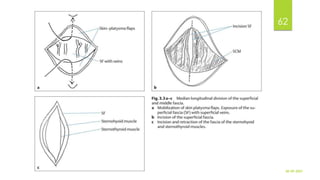
![STRAP MUSCLES & MIDLINE AIRWAY
1. Palpate thyroid cartilage prominence midline
2. Make an incision through cervical fascia in the midline and extend the incision to
expose the full length of the strap muscles. [sternothyroid & sternohyoid]
3. Elevate sternohyoid muscle in midline.
4. Elevate sternothyroid muscle and dissect the thyroid capsule away from it on both sides.
5. This permits adequate digital exploration of entire thyroid gland.
6. Most cases, retract strap m/s: laterally, retract thyroid lobe in opp. direction
7. If gland is unusually large: transect sternothyroid muscle [laryngeal part] in upper third
[Why?]
30-09-2021
63](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-63-320.jpg)
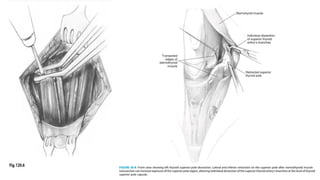











![RLN & Inferior Thyroid artery
• Several approaches
• Triangles [mentioned earlier]
• Thoracic inlet in the RLN Triangle: advantage single nerve trunk [prior to branching]
• Most extra-laryngeal nerves are superior, once its crossed the inferior thyroid artery.
• If found at inferior location, avoid tracing the entire course
• Identify inferior thyroid artery
• Inferior thyroid artery and RLN- intimate foreplay, relations described earlier
• Its typically deep to the artery
• Relationship varies from side to side
• Identification of ITA not only helps in identification of the RLN but also the parathyroid.
30-09-2021
77](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-77-320.jpg)













![BEFORE CLOSURE
1. If appropriate, lobectomy specimen frozen section.
2. Examine neck for nodes [jugular III/IV]
3. Inspect for parathyroid glands
4. Lee found that 11% of 414 thyroidectomy specimens had parathyroid
5. Any presumptive parathyroid should be biopsied for confirmation and then autotransplanted.
30-09-2021
92](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-92-320.jpg)

![POST-OP CARE
Tracheomalacia- on extubation
1. Position: 45 degrees head up for first hours post-op
2. Steroid therapy [i/v] in first 24 hours [analgesia + reduces trans neuropraxia]
3. Antibiotic prophylaxis + analgesia
4. Early mobilization
5. Resume oral intake: complete consciousness, within 4 hours
6. Drain removal <20ml/24h or <10ml/8h
7. Calcium management
8. Post-op VC check
9. Venous thromboembolism prophylaxis: within 24h till discharge
30-09-2021
95](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-95-320.jpg)

![HAEMORRHAGE [1%]
1. Slippage of ligatures
2. Ppt by vigorous coughing or retching in post op period
3. S/S: tachycardia, breathlessness, hypotension
4. Progressive tension hematoma under strap muscles
5. Bedside removal of skin & deeper sutures
6. Later shift to OT and assess
7. BT (sos)
30-09-2021
97](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-97-320.jpg)
![RESPIRATORY OBSTRUCTION
Hematoma– evacuate
Laryngeal edema
Tracheomalacia
Bilateral RLN palsy [fibre-optic laryngoscopy]
30-09-2021
98](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-98-320.jpg)

![HYPOPARATHYROIDISM
• Clinical assessment for HYPOCALCEMIA [clinical signs]
• Asymptomatic: no Rx
• Symptomatic hypocalcemia: Treat with P/O- I/V [Calcium prepn]
• Need for supplementation > 6 months: permanent hypoparathyroidism
• After 2 months: try weaning off from oral calcium and re-assess.
30-09-2021
100](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-100-320.jpg)



![EBSLN INJURY
Mostly unnoticed, more common [as compared to RLN palsy]
Unless professionals [singers, teachers]
Diagnose with fiber-optic laryngoscope
Bowing of VC on paretic side
Videostroboscopy : Assymetric mucosal traveling wave
laryngeal EMG: denervation to cricothyroid muscle
Rx : speech therapy
30-09-2021
104](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-104-320.jpg)
![NERVE INJURIES IN THYROID SURGERY
I. EBSLN injury- not life threatening. Will just lead to
hoarseness
• Inability to sing a high pitch: cricothyroid
II. U/L RLN injury: hoarseness
I. B/L RLN injury- airway obstruction, stridor [emergency]
30-09-2021
105](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-105-320.jpg)






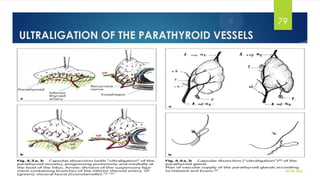
![FLUROSCENT IMAGING AIDS FOR
PARATHYROID IDENTIFICATION
1. Critical for prevention of hypoparathyroidism
2. Detects fluorescence from parathyroid glands
3. Parathyroid tissue auto-fluoroscence in the near infra-red spectrum [285nm]
4. Detection: spectroscopy
5. Adv: non-invasive & avoidance of exogenously administered fluorophore
6. Disadv: limited penetration [few mm], software expertise, visible spectrum light to be turned off
7. Exogenous fluorophore: indocyanine green [i/v]
30-09-2021
112](https://image.slidesharecdn.com/thyroidectomyppt4-211101160412/85/Thyroidectomy-112-320.jpg)