
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Physiology of Blood Lecture
Similar to Physiology of Blood Lecture (20)
Recently uploaded
Recently uploaded (20)
Physiology of Blood Lecture
- 1. Lecture 9-10 Physiology of blood PLAN 1. Components and major functions of blood, and its physical characteristics. 2. The composition and functions of plasma. 3. The characteristics and functions of red blood cells. 4. The structure and functions of hemoglobin. Compounds of hemoglobin with blood gases. 5. The characteristics and functions of platelets. 6. Hemostasis. Its types and mechanisms 7. Blood typing, and the basis for ABO and Rh incompatibilities. 8. Main Physical constants of blood 9. White Blood Cells and their functions. Diagnostic importance of leucogram. 10. Acid-base balance. Chemical and physiological buffer systems of blood. 11. Immunity. Types of immunity and their mechanisms. Principal functions of blood. Transport. Blood transports oxygen and nutrients to the body tissues and carbon dioxide and waste materials from the tissues to the organs of excretion. It also transports hormones from endocrine glands to their target tissues. Acid–base regulation. Blood functions to control acid-base balance through the chemical and physiological buffer systems. For example, high levels of hydrogen ions combine with bicarbonate to form carbonic acid, which dissociates immediately to form carbon dioxide and water; as carbon dioxide is exhaled, blood becomes less acidic, and pH levels stabilize. Thermoregulation. Under conditions of hyperthermia, the blood carries excess heat to the body surface for temperature regulation. Immunity.Leukocytes (white blood cells) are transported in the blood to sites of injury or invasion by disease-causing agents. Hemostasis.Thrombocytes (platelets) and clotting proteins minimize blood loss when a blood vessel is damaged. The composition of blood Blood is composed of a liquid matrix (blood plasma) and several types of formed elements (red blood cells, white blood cells, and platelets) (see.fig). The blood plasma contains a variety of proteins and many other small molecules and ions. Blood minus the formed elements and the clotting proteins is called serum. The hematocrit is the percentage of total blood volume composed of erythrocytes. It ranges from 40% to 54% in men and from 38% to 47% in women. It is measured by centrifuging a blood sample in a capillary tube. For example, if the tube were 100 mm long, and if the packed red blood cells occupied the distal 45 mm, the hematocrit would be 45%. The hematocrit can be changed by anemia and polycythemia. Anemia (low hematocrit) may be caused by a decreased rate of red blood cell production (aplastic anemia) or excessive loss of red blood cells (hemorrhagic or hemolytic anemia) (see table) Polycythemia (high hematocrit) may be caused by excessive red blood cell production The total blood volume makes up about 6-8 percent of the body’s weight. Accordingly, a 70-kilogram person will have from 5 to 6 litres of blood. Circulating blood volume will be lesser than total blood volume, because some amount of blood will be deposited in organs like liver. We use the term hypovolemia if blood volume is less then 6 percent of the body’s weight and - hypervolemia – if it is more then 8 percent of the body’s weight.
- 2. Composition of plasma. The share of plasma accounts for about 55% of the total blood volume. Plasma contains about of 91 % water. The remaining 9% consist of many dissolved substances: - Salts/electrolytes (metal ions) - Proteins - Respiratory gases - Hormones - Nutrients - Waste products. Plasma Proteins (65-85 g/l) include: Albumins (58%) Transport substances such as fatty acids, thyroid hormones, and steroid hormones, take part on establishing of colloid- osmotic stability of blood, form oncotic pressure Globulins (38%) They may be separated by electrophoresis into four types:alpha 1(e.g., fetoprotein, antitrypsin, lipoproteins),alpha 2(e.g., antithrombin, holinesterase),beta(e.g., transferrin, plasminogen, prothymbin), and Gamma (e.g., IgG, IgA, IgM, IgD, IgE; Ig - immunoglobulin). Some globulins, such as antibodies and complement, are part of the immune system. Other globulins like albumin function as transport molecules because they bind to molecules, such as hormones and carry them in the blood throughout the body. Some globulins are clotting factors, which are necessary for the formation of blood clots. Fibrinogen (4%) Molecules that form clots and
- 3. produce long, insoluble strands of fibrin Carbohydrate • The major plasma carbohydrate is glucose (3.3-5.5 mmol/L) . Lipids • Cholesterol (3,8-7,8 mmol/l) • Triglycerides (0,3-1,5 mmol/l) Pigments • Total bilirubin (2,5-17,0 micromol/l) • Direct bilirubin (0-6,0 micromol/l) Waste nitrogenous products • Creatinine (60-120 mmol/l) • uric acid (0,15-0,6 mmol/l) • Urea (3,3-6,5 mmol/l) The main (inorganic) mineral components Total amount is about 0,9% of blood volume • Sodium (Na+), - 133-146 mmol/l • Potassium (K+) – 3,3-5,5 mmol/l • Calcium (Ca++) - 2,0-2,5 mmol/l • Magnesium (Mg++) – 0,75-1,0 mmol/l • Chlorides(Cl⁻) – 96-106 mmol/l • Phosphates (PO4⁻) – 0,8-1,4 mmol/l • Bicarbonates (HCO3⁻) – 24-30 mmol/l Origin, structure, and function of erythrocytes(red blood cells) An erythrocyte, or red blood cell (RBC), is a flexible, biconcave, anucleated cell. RBCs are manufactured at several sites in the body. During embryonic development, erythropoiesis (the manufacture of red blood cells) occurs first in the definitive yolk sac. Production then moves to the liver, spleen, and bone marrow. In children, RBCs are produced in the bone marrow of long bones of the arms and legs. In adults, RBCs are produced in the bon e marrow of the ribs, sternum, vertebrae, and pelvis. The main constituent (about one third by weight) of the RBCs is hemoglobin, and the essential function of these cells is to carry oxygen, reversibly trapped by hemoglobin, to all parts of the body. Biconcave shape of RBC has three important effects on their function: 1. High surface-to-volume ratio • It hepls quickly absorbs and releases oxygen 2. Discs form stacks called rouleau • It provides the smooth flow through narrow blood vessels 3. Discs bend and flex entering small capillaries • It causes 7.8-µm RBC to pass through only 4-µm capillary Red blood cells are the most abundant type of blood cell. Approximately 2.4 million new erythrocytes are produced per second. Approximately a quarter of the cells in the human body are red blood cells. Since RBCs have an elastic membrane, they are able to change their shape when they pass through the capillaries. The cells develop in the bone marrow and circulate for about 100– 120 days in the body before their components are recycled by macrophages. Human red blood cells take on average 20 seconds to complete one cycle of circulation. The normal concentration of RBCs is roughly 4-6 million per mm3 or 4-6* 1012 /l. Many factors can cause fluctuations in erythrocyte number:
- 4. Any condition that decreases oxygen in the body tissues will, by a negative feedback mechanism, increase erythropoiesis, for example, high altitude (30% greater hematocrit at 3,000 m than at sea level), muscle exercise, anemia, or chronic emphysema. Temperature:Increased body temperature increases the number of RBCs. Sex: After puberty, men have a higher hematocrit than women. Age:Infants have a relatively high hematocrit. Time of day:The RBC count is highest in early evening Erythropoiesis is the manufacture of red blood cells. The sequence of cellular differentiation in erythropoiesis is as follows: hemocytoblast →proerythroblast→erythroblast→normoblast→ reticulocyte →erythrocyte. Many biologic active substances are needed for normal erythropoiesis. The most important are Iron, Vitamin B12, Folic acid, copper, cobalt. Hemoglobin and its characteristics. Compounds of hemoglobin with blood gases. Hemoglobin(Hb) consists of globin (four polypeptide chains; fig.) and heme(four Fe+2 and porphyrin molecules). Each erythrocyte contains approximately 280 million hemoglobin molecules. Each iron portion of heme is able to combine with four molecules of oxygen. This means that a single erythrocyte can transport over a billion molecules of oxygen. Depending on structure of globin there are 3 type of hemoglobin: Embryo has HbP (primitive) - (α2ε2) Adults have HbA - (α2β2) Infant have fetal hemoglobin (HbF) - during 1 year (α2γ2) The fetal hemoglobin is different from the adult type It has more affinity to oxygen and can be saturated with oxygen at a lower oxygen tension. If a changing of amino acid order occurs in globin part of hemoglobin molecule, they may lead to formation of pathological types of Hb. For example, sickle cell anemia is developed due to formation HbS when only one amino acid change its place in globin chain of hemoglobin. At this state the erythrocytes change their forms and transport oxygen badly. Normal range of hemoglobin for adults are • adult male 135–180 g/L • adult female 120–160 g/L Carbon dioxide (CO2) and carbon monoxide (CO) also bind to hemoglobin. Hemoglobin, when saturated with oxygen, is called oxyhemoglobin.It is cherry red in color. When oxyhemoglobin loses its oxygen, it becomes bluish purple. Hemoglobin in combination with carbon dioxide is called carbaminohemoglobin. Oxygen and carbon dioxide have distinct carry sites on the Hb molecule. Carbon monoxide combined with Hb is called carboxyhemoglobin. Carbonmonoxide binds to a heme and has 200 times the affinity for the heme that oxygen has. It is Hemoglobin HemeHeme chain 2 chain 2 chain 1 chain 1
- 5. this competitive exclusion of oxygen that makes carbon monoxide so dangerous a gas. Another abnormal compound of hemoglobin is methemoglobin, which contains of Fe+3 instead Fe+2 . Such iron creates strong chemical connection and not able give oxygen to tissues. This conversion occurs if strong oxidants ( for example, cyanide of potassium) accidentally enter into the blood. When disintegrating erythrocytes are phagocytosed in the spleen and liver, the hemoglobin molecule broken down: 1. Hemoglobin →heme+globin 2. Heme→Fe2+porphyrin 3. Globin →protein→amino acids Porphyrin is changed from a ring structure to a straight-chain structure called biliverdin (“green of bile”), which in turn is reduced to the straight-chain bilirubin(“red of bile”). Bilirubin, carried from the liver in the bile, may be excreted in the feces as stercobilinor in the urine as urobilin. Feces and urine owe their brown or yellowish color to these bilirubin products. When yellowish bilirubin accumulates in the blood to an abnormally high degree, it yellows the skin (jaundice). Causes of jaundice include liver disease, excess red blood cell destruction, and bile duct obstruction (feces will be gray). Platelets and their functions. Platelets, or thrombocytes,are small cellular fragments that originate in the bone marrow from a giant cell known as a megakaryocyte.The megakaryocytes form platelets by pinching off bits of cytoplasm and extruding them into the blood. Platelets contain several clotting factors, calcium ions, adenosine diphosphate (ADP), serotonin, and various enzymes; they play an important role in hemostasis (the arrest of bleeding).Normal range of platelets is of : 180-320 x 109 /L. Time of circulation in blood is about of 8-12 days. In the event of a vessel defect or injury, platelets aggregate to form a plug. As they aggregate, they release ADP. The ADP makes the surface of platelets sticky, so that they adhere to the growing layers of aggregated platelets. In addition, thromboxane A2 is released from the surface membranes of aggregating platelets. This prostaglandin derivative further enhances platelet aggregation. The platelet plug aids in reducing blood loss at the site of damage by three mechanisms: (1) physically sealing the vessel defect, (2) releasing chemicals that cause vasoconstriction, and (3) releasing other chemicals that stimulate blood clotting (serotonin, epinephrine, thromboxane A2). The mechanism of hemostasis. There are two types of hemostasis: Vascular-thrombocytes hemostasis : Stoppage of blood loss from the microcirculatory vessels having low blood pressure. Finally – Platelet plug is formed. Coagulatory hemostasis : Stoppage of blood loss from the large vessels having higher blood pressure. Finally – Blood clot is formed The main events of vascular-thrombocytes hemostasis are: Vasoconstriction due to nervous reflex; Adherence of platelets to collagen mediated by Von-Willebrand factor (platelets undergo shape change and release ADP and ATP , ionized calcium, Serotonin, Epinephrine, Thrombaxane A2 from granules); Aggregation of platelets< which results in forming the temporary platelet plug The plasma factors (chemicals), involved in the clotting process, are produced in the liver, and designated by Roman numerals according to their order of discovery. The numerical order, therefore, does not reflect the reaction sequence.
- 6. I - fibrinogen II -prothrombin III- thromboplastin IV- calcium V - labile factor VII- SPCA (serum prothrombin conversion accelerator) VIII- AHF (antihemophilic factor) IX - PTC (plasma thromboplastic component), also called Christmas factor X - Stuart-Prower factor XI - PTA (plasma thromboplastin antecedent) XII- Hageman factor XIII- fibrin stabilizing factor Note:Factor VI is no longer considered a separate entity. Cellular clotting factors are present in the granules of thrombocytes. These factors are released when the platelets undergo degranulation.They are : ADP and ATP Ionized calcium Serotonin Epinephine Thrombaxane A2 Clotting (coagulatory haemostasis) is initiated by two pathways. The intrinsic pathway is activated when blood is exposed to a negatively charged surface, such as that provided by collagen at the site of a wound or by the glass of a test tube. All factors that bring about clotting by means of the intrinsic pathway are present in the blood. The extrinsic pathwayis activated by tissue thromboplastin, which is released when vascular walls or other tissue are damaged. The final steps in both pathways are identical. The main stages of coagulatory haemostasis are: • 1. Activation of prothrombin activator • 2. Prothrombin → Thrombin • 3. Fibrinogen → Fibrin-monomer - fibrin-polymer – cross-linked fibrin-polymer • 4. Retraction of clot.
- 7. Dynamic equilibrium exists between the coagulation system and fibrinolytic system in normal conditions. But if a clot is formed, fibrinolytic system activates and after a few day clots are dissolved by a process called fibrinolysis. Plasminogen is an inactive plasma protein produced by the liver. Thrombin, other clotting factors activated during clot formation, and tissue plasminogen activator (t-PA) released from surrounding tissues can stimulate the conversion of plasminogen to its active form, plasmin. Over a period of a few days, plasmin slowly breaks down the fibrin. Excessive blood clotting can prevent anticoagulants. Citrates and oxalates (organic biochemical molecules) bind calcium, which is essential at several steps in the clotting process. Heparin, a protein released from the liver, prevents the activation of factor IX and interferes with thrombin action. Synthetic anticoagulants Dicoumarol and Coumadin block the formation of prothrombin and factors VII, IX, and X by interfering with vitamin K, which acts as a catalyst in the synthesis of these chemicals in the liver. Some disorders in which there is excessive bleeding. Hemophiliais a hereditary lack, by altered biosynthesis, of a single clotting factor. Lack of VIII causes hemophilia A (classical hemophilia); lack of IX causes hemophilia B (Christmas disease). In vitamin K deficiency,clotting factors are not properly synthesized in the liver. In thrombocytopenia, the concentration of thrombocytes is too low, and the patient may develop hundreds of small hemorrhages (which appear as small purplish blotches on the skin) throughout the body tissues. Blood Types and their significance for clinical practice. Blood types are genetically determined by presence or absence of RBC surface. Although many blood groups are recognized, the ABO and Rh blood groups are the most important for transfusion reactions. The ABO blood group system is used to categorize human blood. ABO antigens appear on the surface of the red blood cells. Type A blood has type A antigens, type B blood has type B antigens, type AB blood has both types of antigens, and type O blood has neither A nor B antigens In addition, plasma from type A blood contains anti-B antibodies, which act against type B antigens,
- 8. whereas plasma from type B blood contains anti-A antibodies, which act against type A antigens. Type AB blood has neither type of antibody, and type O blood has both anti-A and anti-B antibodies. A donor is a person who gives blood, and a recipient is a person who receives blood. Usually, a recipient can receive blood from a donor if they both have the same blood type. For example, a person with type A blood can receive blood from a person with type A blood. There is no ABO transfusion reaction because the recipient has no anti-A antibodies against the type A antigen. On the other hand, if type A blood were donated to a person with type B blood, a transfusion reaction would occur because the person with type B blood has anti-A antibodies against the type A antigen, and agglutination would result. Historically, people with type O blood have been called universal donors because they usually can give blood to the other ABO blood types without causing an ABO transfusion reaction. Their red blood cells have no ABO surface antigens and, therefore, do not react with the recipient’s anti-A or anti-B antibodies. For example, if type O blood is given to a person with type A blood, the type O red blood cells do not react with the anti-B antibodies in the recipient’s blood. In a similar fashion, if type O blood is given to a person with type B blood, there is no reaction with the recipient’s anti-A antibodies. The term universal donor is misleading, however. There are two ways in which the transfusion of type O blood can produce a transfusion reaction. First, mismatching blood groups other than the ABO blood group can cause a transfusion reaction. Second, antibodies in the donor’s blood can react with antigens in the recipient’s blood. For example, type O blood has anti-A and anti-B antibodies. If type O blood is transfused into a person with type A blood, the anti-A antibodies (in the type O blood) react against the A antigens (on the red blood cells in the type A blood). Usually such reactions are not serious because the antibodies in the donor’s blood are diluted in the large volume of the recipient’s blood, and few reactions take place. Another important blood group is the Rh blood group, so named because it was first studied in the rhesus monkey. People are Rh-positive if they have a certain Rh antigen (the D antigen) on the surface of their red blood cells, and people are Rh-negative if they do not have this Rh antigen.About of 85% of people are Rh+ and about of 15% are RH-. Rh- conflict and its prevention. Antibodies against the Rh antigens do not develop unless an Rh-negative person is exposed to Rh-positive red blood cells. This can occur through a transfusion or by the transfer of blood across the placenta to a mother from her fetus. When an Rh- negative person receives a transfusion of Rh-positive blood, the recipient becomes sensitized to the Rh antigens and produces anti-Rh antibodies. If the Rh-negative person is unfortunate enough to receive a second transfusion of Rh-positive blood after becoming sensitized, a transfusion reaction results. Rh incompatibility can pose a major problem in some pregnancies when the mother is Rh- negative and the fetus is Rh- positive. If fetal blood leaks through the placenta and mixes with the mother’s blood, the mother becomes sensitized to the Rh antigen. The mother produces anti-Rh antibodies that cross the placenta and cause agglutination and hemolysis of fetal red blood cells. This disorder is called hemolytic disease of the newborn (HDN),or erythroblastosis fetalis, and it can be fatal to the fetus. In the mother’s first pregnancy, there is often no problem. The leakage of fetal blood is usually the result of a tear in the placenta that takes place either late in the pregnancy or during delivery. Thus, there is not enough time for the mother to produce enough anti Rh antibodies to harm the fetus. If sensitization occurs, however, it can cause problems in a subsequent pregnancy in two ways. First, once a woman is sensitized and produces anti-Rh antibodies, she may continue to produce the antibodies throughout her life. Thus, in a subsequent pregnancy, anti-Rh antibodies may already be present. Second, and especially dangerous in a subsequent pregnancy with an Rh-positive fetus, if any leakage of fetal blood into the mother’s blood occurs, she rapidly produces large amounts of anti-Rh antibodies, and HDN develops. Therefore, the levels of anti-Rh antibodies in the mother should be tested. If they are too high, the fetus should be tested to determine the severity of the HDN. In severe cases, a transfusion to replace lost red blood cells can be performed through the umbilical cord, or the baby can be delivered if mature enough.
- 9. Prevention of HDN is often possible if the Rh-negative mother is given an injection of a specifi c type of antibody preparation, called Rho(D) immune globulin (RhoGAM). Th e injection can be given during the pregnancy, before delivery, or immediately after each delivery, miscarriage, or abortion. Th e injection contains antibodies against Rh antigens. The injected antibodies bind to the Rh antigens of any fetal red blood cells that may have entered the mother’s blood. This reatment inactivates the fetal Rh antigens and prevents sensitization of the mother. However, if sensitization of the mother has already occurred, the treatment is ineffective. Blood Type Testing. Three different type of serum are needed for blood type testing: anti A, anti B and anti D. Which of this serum contains antibodis against of corresponding antigen. When these antibodies are encountered with their antigen, the agglutination occurs. It is shown on the figure White blood cells (WBC – normal range 4-9*109 per liter) White blood cells, or leukocytes, are spherical cells that lack hemoglobin. White blood cells form a thin, white layer of cells between plasma and red blood cells when the components of blood are separated from each other. They are larger than red blood cells, and each has a nucleus. Although white blood cells are components of the blood, the blood serves primarily as a means to transport these cells to other tissues of the body. White blood cells can leave the blood and move by ameboid movement through the tissues. Two main functions of white blood cells are: (1) to protect the body against invading microorganisms and (2) to remove dead cells and debris from the tissues by phagocytosis. Anti-A Anti-B Anti-D Blood type B+ AB+ O– A+
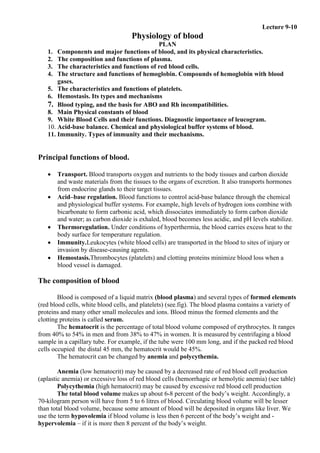
- 10. Each white blood cell type is named according to its appearance in stained preparations. Those containing large cytoplasmic granules are granulocytes and those with very small granules that cannot be easily seen with the light microscope are agranulocytes There are three kinds of granulocytes: neutrophils, basophils, and eosinophils. Neutrophils, (2.5–7.5 x 109 /L) the most common type of white blood cells, have small cytoplasmic granules that stain with both acidic and basic dyes. Th eir nuclei are commonly lobed, with the number of lobes varying from two to four. Neutrophils usually remain in the blood for a short time (10–12 hours), move into other tissues, and phagocytize microorganisms and other foreign substances. Neutrophils also secrete chemicals that promote inflammation and a class of enzymes called lysozymes, which are capable of destroying certain bacteria. Pus is an accumulation of dead neutrophils, cell debris, and fl uid at sites of infections. Basophils (0.01-0.1 x 109 /L), the least common of all white blood cells, contain large cytoplasmic granules that stain blue or purple with basic dyes (see table 16.2). Basophils release histamine and other chemicals that promote inflammation. They also release heparin, which prevents the formation of clots. Blast Cells Progenitor Cells Lymphoid Stem CellsMyeloid Stem Cells HemocytoblastsRed bone marrow Proerythroblast Erythroblast stages Ejection of nucleus Reticulocyte Erythrocyte Red Blood Cells (RBCs) Megakaryocyte Platelets Myelocytes Band Cells Agranulocytes Monoblast Promonocyte Monocyte Lymphoblast Prolymphocyte Lymphocyte Myeloblast Basophil Eosinophil Neutrophil Granulocytes White Blood Cells (WBCs)
- 11. Eosinophils (0.2–0.8 x 109 /L ) contain cytoplasmic granules that stain bright red with eosin, an acidic stain. Many have a two-lobed nucleus. Eosinophils release chemicals that kill multicellular parasites, which are too large to be ingested and killed by phagocytosis. They also release chemicals that promote inflammation. Increased numbers of eosinophils is a characteristic of chronic allergic inflammation, such as occurs in asthma. There are two kinds of agranulocytes: lymphocytes and monocytes. Lymphocytes (1.5–3.5 x 109 /L) are the smallest of the white blood cells. The cytoplasm of lymphocytes consists of only a thin, sometimes imperceptible ring around the nucleus. Lymphocytes originate in red bone marrow and migrate through the blood to lymphatic tissues, where they can proliferate and produce more lymphocytes. There are several types of lymphocytes, and they play an important role in immunity. For example, B cells can be stimulated by bacteria or toxins to divide and form cells that produce proteins called antibodies. Antibodies can attach to bacteria and activate mechanisms that result in the destruction of the bacteria. T cells protect against viruses and other intracellular microorganisms by attacking and destroying the cells in which they are found. In addition, T cells are involved in the destruction of tumor cells and tissue graft rejections. Monocytes (0.2–0.8 x 109 /L ) are the largest of the white blood cells. After they leave the blood and enter tissues, monocytes enlarge and become macrophages, which phagocytize bacteria, dead cells, cell fragments, and any other debris within the tissues. An increase in the number of monocytes is often associated with chronic infections. Monocytes also release chemicals that promote inflammation. In addition, macrophages can process and present phagocytized foreign substances to lymphocytes, which results in activation of the lymphocytes. A blood leucocyte profile is called leucogram. It provides information on total leucocyte count, differential leucocyte count and leucocyte morphology. Normal leucogram in adults is shown below Total N.of leucocytes Juvenile neutrophils Immature neutrophils Segmented neutrophils Eosinophils Basophils Lymphocytes Monocytes Normal Range 4-9 x 109 /L 1% 6% 60% 0.5-5% 0- 1% 18-37% 3-11% If the amount of young neutrophils is higher then normal value but the amount of mature neutrophils is very low , then we conclude as :shift to left ( for example Infection by pathogen). If the amount of mature neutrophil is normal but the amount of young neutrophils is zero , then we conclude as: shift to right (perhaps it is Problem in bone marrow). Normally in adults neutrophil level is higher than the level of lymphocytes. At birth, the amount of neutrophils and lymphocytes are in the ratio as in adults. At age of 3 - 5 days, lymphocytes increase and neutrophils decrease and remains the same until 3– 5 years, and then again becomes normal. This is called the physiological cross of leucocytes in ontogenesis. Becase of physiological cross the leucogram in children at age from 3-5 days to 3-5 years is not the same as in adults. Below is list some diseases that cause increases in the various leukocytes types. Neutrophils: appendicitis, pneumonia, tonsillitis and other bacterial infections; Eosinophils: hay fever, asthma, parasitic infestations; Basophils: smallpox, nephritis, myxedema; Lymphocytes: whooping cough, mumps, mononucleosis; Monocytes:tuberculosis, typhus. Main Physical constants of blood • Osmotic pressure (280-300 mosm/l) • Oncotic pressure (20-25 mm Hg) • Blood pH (7,35-7,45)
- 12. • Viscosity (3-5 unit) • Erythrocyte sedimentation rate (ESR) – • Males – 2-10 mm/hour • Females – 2-15 mm/hour) Osmotic pressure is defined as the minimum amount of pressure needed to prevent osmosis. Dissolved particles maintain the osmotic pressure. Among them, the most active is NaCl (0.9 % solution is isotonic) and also glucose (5 % solution is isotonic). In hypotonic solution swelling and bursting of blood cells occurs. In hypertonic solution shrinkage of cells occurs. Osmotic resistance of RWC’s is erythrocyte resistance to the action of hypotonic solutions. It can be measured as a NaCl solution concentration at which complete hemolysis of erythrocytes occurs. Normal value correspond to 0.35 (maximal resistance) - 0.45 (minimal resistance) % of NaCl solution. Oncotic pressure, or colloid osmotic pressure, is a form of osmotic pressure exerted by blood plasma proteins. It usually tends to pull water (fluid) into the circulatory system (capillaries). It is the opposing force to hydrostatic pressure. Its normal value is : 0.03-0.04 atm. (or) 20-25 mm Hg Blood viscosity can be described as the thickness and stickiness of blood. It is a measure of the resistance of blood to flow. The viscosity of blood is 4-5 times more than that of pure water by 20o of C (based on time taken for the flow of both in a tube). It is directly proportional to RBCs count and plasma proteins concentration. The erythrocyte sedimentation rate (ESR), is the rate at which red blood cells sediment in a period of one hour. It is a common hematology test. Factors influencing the ESR : Plasma proteins (mainly fibrinogen and globulins) negative charge of the erythrocytes (zeta potential). Increased ESR may be due to pregnancy (second half), inflammation, cancer. Decreased ESR may be due to: polycytaemia; sickle cell anemia, hereditary spherocytosis, congestive heart failure. Acid-Base Equilibrium. The term acid–base equilibrium (balance) refers to the precise regulation of free (that is, unbound) hydrogen ion (H+) concentration in the body fluids. To indicate the concentration of a chemical, its symbol is enclosed in square brackets. Thus, [H+] designates H+ concentration. The pH designation is used to express [H+].The concept of pH was developed to express the low value of [H+] more conveniently. Specifically, pH equals the logarithm (log) to the base 10 of the reciprocal of [H+]. This formula may seem intimidating, but you only need to glean one important point from it: because [H+] is in the denominator, a high [H+] corresponds to a low pH, and a low [H+] corresponds to a high pH. The greater the [H+], the larger the number by which 1 must be divided, and the lower the pH.
- 13. The pH of arterial blood is normally 7.45 and the pH of venous blood is 7.35, for an average blood pH of 7.4. The pH of venous blood is slightly lower (more acidic) than that of arterial blood because H+ is generated by the formation of H2CO3 from CO2 picked up at the tissue capillaries. Acidosis exists whenever blood pH falls below 7.35, whereas alkalosis occurs when blood pH is above 7.45 The role of pH in body metabolism. Hydrogen ion concentration exerts a marked influence on enzyme activity. Even slight deviations in [H+] alter the shape and activity of protein molecules. Because enzymes are proteins, a shift in the body’s acid–base balance disturbs the normal pattern of metabolic activity catalyzed by these enzymes. Three lines of defense against changes in [H+] operate to maintain [H+] of body fluids at a nearly constant level despite unregulated input: 1. the chemical buffer systems, 2. the respiratory mechanism of pH control, and 3. the renal mechanism of pH control. We now look at each of these methods. Mechanism of chemical buffer system action. A chemical buffer system is a mixture in a solution of two chemical compounds that minimize pH changes when either an acid or a base is added to or removed from the solution. A buffer system consists of a pair of substances involved in a reversible reaction—one substance that can yield free H+ as the [H+ ] starts to fall and another that can bind with free H+ (thus removing it from solution) when [H+ ] starts to rise. An important example of such a buffer system is the carbonic acid–bicarbonate (H2CO3:HCO3 – ) buffer pair, which is involved in the following reversible reaction: When a strong acid such as HCl is added to an unbuffered solution, all the dissociated H+ remains free in the solution. In contrast, when HCl is added to the buffer solution the HCO3– immediately binds with the free H+ to form H2CO3This weak H2CO3 dissociates only slightly compared to the marked reduction in pH that occurred when the buffer system was not present and the additional H+ remained unbound. In the opposite case, when the pH of the solution starts to rise from the addition of base or loss of acid, - yielding member of the buffer pair, H2CO3, releases H+ to minimize the rise pH. Chemical buffer systems of the blood. The body has four buffer systems: (1) the bicarbonate buffer system, (2) the protein buffer system, (3) the hemoglobin buffer system, and (4) (the phosphate buffer system. The hydrocarbonate buffer system.
- 14. The H2CO3:HCO3 – buffer pair is the primary extracellular fluid (ECF) buffer for noncarbonic acids. It is the most important buffer system in the ECF for buffering pH changes brought about by causes other than fluctuations in CO2-generated H2CO3. It is an effective ECF buffer system for two reasons. First, H2CO3and HCO3 – are abundant in the ECF, so this system is readily available to resist changes in pH. Second, and more importantly, each component of this buffer pair is closely regulated. The kidneys regulate HCO3– , and the respiratory system regulates CO2, which generates H2CO3 The Protein Buffer System. The protein buffer system is primarily important intracellularly. The most plentiful buffers of the body fluids are the proteins, including the intracellular proteins and the plasma proteins. Proteins are excellent buffers, because they contain both acidic (COOH) and basic (NH2) groups that can give up or take up H+ . Quantitatively, the protein system is most important in buffering changes in [H+ ] in the intracellular fluid (ICF) because of the sheer abundance of the intracellular proteins. Hemoglobin buffer system This system consists of the pair oxyhemoglobin as weak acid and deoxyhemoglobin as weak base. It operates only during breathing, when permanent transformation of these two forms of hemoglobin occurs. In lungs hemoglobin buffer system prevents alkalosis and in tissues – acidosis. The Phosphate Buffer System The phosphate buffer system is an important urinary buffer. It consists of an acid phosphate salt that can donate a free H+ when the [H+ ] falls (H2PO4 - ) and a basic phosphate salt that can accept a free H+ when the [H+ ] rises (HPO4 - ). Even though the phosphate pair is a good buffer, its concentration in the ECF is rather low, so it is not very important as an ECF buffer. Because phosphates are most abundant within the cells, this system contributes significantly to intracellular buffering, being rivaled only by the more plentiful intracellular proteins. Physiological Buffer Systems. The respiratory system regulation of acid-base balance is a physiological buffering system. There is a reversible equilibrium between dissolved carbon dioxide and water on the one hand and carbonic acid, the hydrogen and bicarbonate ions on the other hand. During carbon dioxide unloading, hydrogen ions are incorporated into water. When hypercapnia or rising plasma H+ occurs: deeper and more rapid breathing expels more carbon dioxide and hydrogen ion concentration is reduced. Alkalosis causes slower, more shallow breathing, causing H+ to increase. Respiratory system impairment causes acid-base imbalance (respiratory acidosis or respiratory alkalosis). The kidneys are a powerful third line of defense against changes in [H+ ]. The kidneys control the pH of body fluids by adjusting different interrelated factors: (1) Antiport (H+ excretion coupled with HCO3 - reabsorption ) , (2) Regulation of HCO3 – reabsorption and excretion by urine (3) ammonia (NH4 + ) secretion. 4) Excretion of the acid phosphate or base phosphate by urine. The kidneys require hours to days to compensate for changes in body-fluid pH, compared to the immediate responses of the buffer systems and the few minutes of delay before the respiratory system responds. However, the kidneys are the most potent acid–base regulatory mechanism; they can not only vary removal of H+ from any source but also can variably conserve or eliminate HCO3 – depending on the acid–base status of the body. By simultaneously removing acid (H+ ) from and adding base (HCO3 – ) to body fluids, the kidneys are able to restore the pH toward normal more effectively than the lungs, which can adjust only the amount of H+ -forming CO2 in the body Evaluation of acid-base balance disturbances.
- 15. Diagnosis of acid-base disturbances includes measuring: 1. plasma pH N. 7,35-7,45 2. PCO2 N. 35-45 mm Hg 3. Plasma bicarbonate N. 22-28 mmol/l The typical changes of these parameters by different acid-base disturbances are presented in the table. decrease in pH decrease in [HCO3 - ]Metabolic Acidosis - decrease in PCO2 decrease in pH increase in [HCO3 - ]Respiratory Acidosis - increase in PCO2 increase in pH increase in [HCO3 - ]Metabolic Alkalosis - increase in PCO2 increase in pH decrease in [HCO3 - ]Respiratory Alkalosis - decrease in PCO2 The acid-base disturbances can be fully compensated, partly compensated or decompensated. The schema below gives the strategy for evaluation of these. Fully compensated pH = 7,35-7,45 Partly compensated pH = 7,2-7,35 decompensated pH < 7,2 Partly compensated pH = 7,45-7,60 decompensated pH > 7,6
- 16. Immunity and its mechanisms. Immunity is the ability to resist damage from pathogens and internal threats, if they contain genetically foreign proteins and nucleic acids. Such genetically foreign substances are called antigens. Immunity functions to prevent the entry of antigens into the body and to eliminate them if they do. Immunity is realised by immune system, which consists of central immune organs (bone marrow and thymus) and peripheral immune structures (the tonsils, lymph nodes, spleen, diffuse lymphatic tissue and lymphatic nodules located within internal organs). The key to a healthy immune system is its remarkable ability to distinguish between the body’s own cells—self—and foreign cells—nonself. The body’s immune defenses normally coexist peacefully with cells that carry distinctive “self” marker molecules. But when immune defenders encounter cells or organisms carrying markers that say “foreign,” they quickly launch an attack. Major histocompatibility complex (MHC) or human leukocyte antigens (HLA) (because they were first identified on white blood cells) is a group of membrane proteins, which help T cells recognize that an antigen is foreign, not self. Class I MHC antigens are in cell membranes of all body cells except red blood cells. Class II MHC antigens are on the surfaces of antigen-presenting cells (microphages), thymus cells, and activated T cells. Some immune mechanisms are general and protect against many types of pathogens, providing innate (nonspecific) defense. They function the same way regardless of the pathogen or the number of exposures. These mechanisms include species resistance, mechanical barriers, chemical barriers (enzyme action, interferon, and complement), natural killer cells, inflammation, phagocytosis, and fever. Other defense mechanisms are very precise, targeting specific pathogens with an adaptive(specific) defense, or immunity. These more directed responses are carried out by specialized lymphocytes that recognize foreign molecules (nonself antigens) in the body and act against them. Innate and adaptive defense mechanisms work together to protect the body against infection. While the innate defenses respond rapidly, slower-to-respond adaptive defenses begin as well. Innate (nonspecific) defences include: Species resistance refers to the fact that a species may be resistant to diseases that affect other species because its cells do not have receptors for the pathogen or its tissues do not provide the temperature or chemical environment that a particular pathogen requires. For example, humans are resistant to certain forms of malaria and tuberculosis that affect birds. Mechanical barriers. The skin and mucous membranes lining the passageways of the respiratory, digestive, urinary, and reproductive systems create mechanical barriers that prevent the entrance of some infectious agents. As long as these barriers remain intact, many pathogens are unable to penetrate them. Hair traps infectious agents associated with the skin and mucous membranes and sweat and mucus rinse away microorganisms. Tears, saliva, and urine also wash away organisms before they become firmly attached. These barriers provide a first line of defense. Chemical barriers are the second line of defense . Enzymes in body fluids provide a chemical barrier to pathogens. Gastric juice, for example, contains the protein-splitting enzyme pepsin and has a low pH due to hydrochloric acid in the stomach. The combined effect of pepsin and hydrochloric acid kills many pathogens that enter the stomach. Similarly, tears contain the enzyme lysozyme, which destroys certain bacteria on the eyes. The accumulation of salt from perspiration also kills certain bacteria on the skin. Interferons are hormonelike peptides that lymphocytes and fibroblasts produce in response to viruses or tumor cells. Once released from a virus-infected cell, interferon binds to receptors on uninfected cells, stimulating them to synthesize proteins that block replication of a variety of viruses. Thus, interferon’s effect is nonspecific. Interferons also stimulate phagocytosis and enhance the activity of other cells that help to resist infections and the growth of tumors. Other antimicrobial biochemicals are defensins and collectins. Defensins are peptides produced by neutrophils and other types of granular white blood cells in the intestinal epithelium,
- 17. the urogenital tract, the kidneys, and the skin. Recognition of a nonself cell surface or viral particle triggers the expression of genes that encode defensins. Some defensins make holes in bacterial cell walls and membranes, crippling the microbes. Collectins are proteins that provide broad protection against bacteria, yeasts, and some viruses. These proteins home in on slight differences in the structures and arrangements of sugars that protrude from the surfaces of pathogens. Complement is a group of proteins (complement system), in plasma and other body fluids, that interact in a series of reactions or cascade. Complement activation can rapidly occur by the classical pathway when a complement protein binds to an antibody attached to its specific antigen or more slowly by the alternative pathway triggered by exposure to foreign antigens, in the absence of antibodies. Activation of complement stimulates inflammation, attracts phagocytes, and enhances phagocytosis. Natural killer (NK) cells .Natural killer (NK)cells are a small population of lymphocytes that are distinctly different from the lymphocytes that provide adaptive defense mechanisms. NK cells defend the body against various viruses and cancer cells by secreting cytolytic (“cell-cutting”) substances called perforins that lyse the cell membrane, destroying the infected cell. NK cells also secrete chemicals that enhance inflammation. Inflammation produces localized redness, swelling, heat, and pain. The redness is a result of blood vessel dilation that increases blood fl ow and volume in affected tissues (hyperemia). This effect, coupled with an increase in permeability of nearby capillaries and subsequent leakage of protein-rich fluid into tissue spaces, swells tissues (edema). The heat comes as blood enters from deeper body parts, which are warmer than the surface. Pain results from stimulation of nearby pain receptors. Most inflammation is a tissue response to pathogen invasion, but physical factors (heat, ultraviolet light) or chemical factors (acids, bases) can also cause it. Phagocytosis removes foreign particles from the lymph as it moves from the interstitial spaces to the bloodstream. Phagocytes in the blood vessels and in the tissues of the spleen, liver, or bone marrow usually remove particles that reach the blood. The most active phagocytic cells of the blood are neutrophils and monocytes. Chemicals released from injured tissues attract these cells (chemotaxis). Neutrophils engulf and digest smaller particles; monocytes phagocytize larger ones. Monocytes that leave the blood become macrophages, which may be free or fixed in various tissues including lymph nodes, the spleen, the liver, and the lungs, or attached to the inner walls of blood and lymphatic vessels. A macrophage can engulf up to 100 bacteria, compared to the twenty or so bacteria that a neutrophil can engulf. Monocytes, macrophages, and neutrophils constitute the mononuclear phagocytic system (reticuloendothelial system). A fever is a nonspecific defense that offers powerful protection. A fever begins as a viral or bacterial infection stimulates lymphocytes to proliferate, producing cells that secrete a substance called interleukin-1(IL-1), more colorfully known as endogenous pyrogen IL-1 raises the thermoregulatory set point in the brain’s hypothalamus to maintain a higher body temperature. Fever indirectly counters microbial growth because higher body temperature causes the liver and spleen to sequester iron, which reduces the level of iron in the blood. Bacteria and fungi require iron for normal metabolism, so their growth and reproduction in a fever-ridden body slows and may cease. Also, phagocytic cells attack more vigorously when the temperature rises. For these reasons, low-grade fever of short duration may be a desired natural response, not a symptom to be treated aggressively with medications. Adaptive (specific) defences is resistance to specific pathogens or to their toxins or metabolic by-products. An immune response is based upon the ability to distinguish molecules that are part of the body (“self”) from those that are not (“nonself,” or foreign). Lymphocytes and macrophages that recognize specific nonself antigens carry out adaptive immune responses. This responses have two interconnected branches: cellular and humoral. T Cells and the Cellular Immune Response. During fetal development, red bone marrow releases unspecialized precursors of lymphocytes into the circulation. About half of these cells reach the thymus, where they remain for a time. Here, these thymocytes specialize into T cells. (“T” refers to thymus-derived lymphocytes.) Later, some of these T cells constitute 70% to 80% of the circulating lymphocytes in blood. Other T
- 18. cells reside in lymphatic organs and are particularly abundant in the lymph nodes, the thoracic duct, and the white pulp of the spleen. Other lymphocytes remain in the red bone marrow until they differentiate fully into B lymphocytes, or B cells. (Historically, the “B” stands for bursa of Fabricius, an organ in the chicken where these cells were discovered.) The blood distributes B cells, which constitute 20% to 30% of circulating lymphocytes. B cells settle in lymphatic organs along with T cells and are abundant in lymph nodes, the spleen, bone marrow, and the intestinal lining. Each person has millions of varieties of T and B cells. The members of each variety originate from a single early cell, so they are all alike, forming a clone of cells (genetically identical cells originating from division of a single cell). The members of each variety have a particular type of antigen receptor on their cell membranes that can respond only to a specific antigen. A lymphocyte must be activated before it can respond to an antigen. T cell activation requires processed fragments of antigen attached to the surface of another type of cell, called an antigen-presenting cell (accessory cell). Macrophages, B cells, and several other cell types can be antigen-presenting cells.T cell activation begins when a macrophage phagocytizes a bacterium, digesting it in its lysosomes. Some bacterial antigens exit the lysosomes and move to the macrophage’s surface. MHC antigens help T cells recognize that an antigen is foreign, not self. Activated T cells interact directly with the antigen-presenting cell. Such cell-to-cell contact is called the cellular immune response, or cell-mediated immunity. T cells (and some macrophages) also synthesize and secrete polypeptides called cytokines that enhance certain cellular responses to antigens. For example, interleukin-1 and interleukin-2 stimulate synthesis of several cytokines from other T cells. In addition, interleukin-1 helps activate T cells, whereas interleukin-2 causes T cells to proliferate. Other cytokines called colony-stimulating factors (CSFs) stimulate production of leukocytes in the red bone marrow, cause B cells to grow and mature, and activate macrophages. Certain cytokine combinations shut off the immune response. Table below summarizes several cytokine types.
- 19. T cells may also secrete toxins that kill their antigen bearing target cells, growth-inhibiting factors that prevent target cell growth, or interferon that inhibits the proliferation of viruses and tumor cells. Several types of T cells have distinct functions. A specialized type of T cell, called a helper T cell, becomes activated when its antigen receptor combines with displayed foreign antigen. Once activated, the helper T cell stimulates the B cell to produce antibodies specific for the displayed antigen. A type of helper T cell called a CD4 cell is the prime target of HIV, the virus that causes AIDS. (CD4 stands for the “cluster of-differentiation” antigen it bears that enables it to recognize a macrophage displaying a foreign antigen). Considering the role of CD4 helper T cells as key players in establishing immunity—they stimulate B cells and secrete cytokines—it is no wonder that harming them destroys immunity. Another type of T cell is a cytotoxic T cell, which recognizes and combines with nonself antigens that cancerous cells or virally infected cells display on their surfaces near certain MHC proteins. Cytokines from helper T cells activate the cytotoxic T cell. Next the cytotoxic T cell proliferates, enlarging its clone of cells. Cytotoxic T cells then bind to the surfaces of antigen- bearing cells, where they release perforin - protein that cuts pore like openings, destroying these cells. In this way, cytotoxic T cells continually monitor the body’s cells, recognizing and eliminating tumor cells and cells infected with viruses. Certain cytotoxic T cells, called CD8 T cells, give rise to memory T cells that provide for future immune protection. When a CD8 T cell contacts an antigen-presenting cell, it contorts into a dumbbell shape. The side of the dumbbell that contacts the antigen-presenting cell accumulates different receptors and other proteins from the side facing farthest from the provoking antigen. When the CD8 T cell divides, the daughter cell that was the part of the original cell closest to the antigen becomes an active cytotoxic T cell. The daughter cell farther from the antigen becomes a memory T cell. As its name implies, a memory T cell does not respond to an initial exposure to an antigen, but upon subsequent exposure immediately divides and differentiates into a cytotoxic T cell. This response usually vanquishes the pathogen before it can cause the body to produce signs and symptoms of disease. B Cells and the Humoral Immune Response. Sometimes a B cell may become activated when it encounters an antigen whose molecular shape fits the shape of the B cell’s antigen receptors. In response to the receptor-antigen combination, the B cell divides repeatedly, expanding its clone. However, most of the time B cell activation requires T cell “help.” When an activated helper T cell encounters a B cell already combined with an identical foreign antigen, the helper cell releases certain cytokines. These cytokines stimulate the B cell to proliferate, thus enlarging its clone of antibody-producing cells (fig. 16.18). The cytokines also attract macrophages and leukocytes into inflamed tissues and help keep them there.
- 20. Some members of the activated B cell’s clone differentiate further into memory cells. Like memory T cells, these memory B cells respond rapidly to subsequent exposure to a specific antigen. Other members of the activated B cell’s clone differentiate further into plasma cells, which produce and secrete large globular proteins called antibodies or immunoglobulins similar in structure to the antigen-receptor molecules on the original B cell’s surface). These antibodies can combine with the antigen on the pathogen and react against it. A plasma cell is an antibody factory, as evidenced by its characteristically huge Golgi apparatus. At the peak of an infection, a plasma cell may produce and secrete 2,000 antibody molecules per second! Body fluids carry antibodies, which then react in various ways to destroy specific antigens or antigen-bearing particles. This antibody-mediated immune response is called the humoral immune response(“humoral” refers to fluid). T cells can suppress antibody formation by releasing cytokines that inhibit B cell function. A single type of B cell carries information to produce a single type of antibody. However, different B cells respond to different antigens on a pathogen’s surface. Therefore, an immune response may include several types of antibodies manufactured against a single microbe or virus. This is called a polyclonal response. Primary and secondary immune responses. When B cells or T cells become activated after first encountering the antigens for which they are specialized to react, their actions constitute a primary immune response. During such a response, plasma cells release antibodies (IgM, followed by IgG) into the lymph. The antibodies are transported to the blood and then throughout the body, where they help destroy antigen-bearing agents. Production and release of antibodies continues for several weeks. After a primary immune response, some of the B cells produced during proliferation of the clone remain dormant and serve as memory cells. If the identical antigen is encountered in the future, the clones of these memory cells enlarge, and they can respond rapidly with IgG to memory B cells with memory T cells produce a secondary immune response. In lymph nodes, follicular dendritic cells may help memory by harboring and slowly releasing viral antigens after an initial infection.