
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Approaches to Brainstem
Similar to Approaches to Brainstem (20)
Recently uploaded
Recently uploaded (20)
Approaches to Brainstem
- 1. Approaches to the Brainstem
- 6. How to approach the brain stem ? • Possible transcranial routes • Approaching lesions in the brainstem • Possible safe entry zones Intent of management? • Biopsy • Decompression • Total excision
- 7. Approach selection Preoperative Planning • The ultimate success depends largely on preoperative planning and preparation. • Selection of the proper approach - a key component of preparation. • Ideally, the approach uses - the shortest distance, although this is not possible in every case. minimally disturbing adjacent neural pathways.
- 8. Intraoperative monitoring • Cranial nerves EMG monitoring -III IV V VI VII VIII IX X XI XII BAEP • MEP/SSEP
- 13. • IOM - the mapping of cranial nerve nuclei. • Based on intraoperative electrophysiological findings and the compound muscle action potentials from related muscles. • Facilitates the identification of “safe” entry zones to the brainstem. • Useful in midline tumors or floor of the fourth ventricle. • Not useful for ventrally or laterally located lesions.
- 14. Anesthesia in the Setting of Brainstem IOM • Ultra-short-acting paralytics limited to induction • Constant infusion of iv agents for steady state of anesthesia • Avoidance of agents that degrade IOM – Hypothermia, hypotension inhaled halogenated anesthetic agents intermittent injection of intravenous anesthetics
- 15. Method - • Starting with a current of 0.2-0.3 mA, probe is applied to an area of interest for no longer than 5 seconds and is moved at 1-mm intervals to create a functional map of the floor of the fourth ventricle. • Distortion of anatomy by tumor mapped. • Update map during resection. • MEPs of the corticospinal tract can be used for monitoring descending motor tracts during resections of brainstem tumors. • SSEP useful for understanding surgery’s impact on sensory function.
- 17. Image Guidance for Brainstem Surgery • The use of image guidance often directs intra- operative decision making as to the location of the lesion and the boundary of pathology with normal tissues. • In cases where the lesion does not abut a pial surface, neuronavi- gation can assist with the selection of entry points.
- 18. Surgical Tools for Brainstem Surgery • Because the visual axis and light source of the microscope are 3° to 6° apart, depending on the focal length used, the small deep exposure is frequently poorly illuminated. • Lighted suction and bipolar devices eliminate this problem. • Use of dynamic retraction. Bayonetted lighted bipolar forceps
- 19. The Two-Point Method • To guide the surgical approach selection for deep- seated lesions. • The surgeon places a point at the center of the lesion (Point A). • A second point (Point B) is selected where the lesion most closely approximates a pial or an ependymal surface. • A straight line is drawn from Point A to Point B and then extended to the skull. • This line defines the optimal trajectory for approaching the lesion.
- 20. Application of two-point method with selection of an alternative
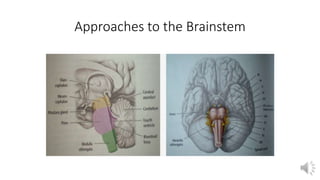
- 21. Approaches to Brainstem Schematic drawing illustrating the most common surgical approaches used for different areas of the brainstem.
- 23. A solid/cystic anterior mesencephalic lesion with expansion towards the interpeduncular cistern, resection done by fronto- orbito zygomatic approach
- 24. Tumors located at the central portion of the midbrain and growing towards the pineal region. Infratentorial supracerebellar approach.
- 25. Tumor in the quadrigeminal plate growing towards the fourth ventricle. Transtentorial occipital approach
- 26. A large tumor growing towards third and fourth ventricle. Approached by combined infratentorial supracerebellar followed by subocciptal telovelar approach.
- 27. Endoscopic access to tumors located in the anterior and superior portion of the midbrain.
- 28. A large lesion in the anterior and superior portion of the pons, approached via orbito-fronto zygomatic via the supratrigeminal entry zone.
- 29. Superior and posterior pontine tumor approached via suboccipital telovelar approach with the point of entry into the pons through the suprafacial triangle.
- 30. A large tumor anterior to the medulla. The far lateral approach and trans- olivary point of entry used for resection .
- 31. Thirteen zones were selected: 1) anterior mesencephalic zone 2) lateral mesencephalic sulcus 3) intercollicular region 4) peritrigeminal zone 5) supratrigeminal zone 6) lateral pontine zone 7) supracollicular zone 8) infracollicular zone 9) median sulcus of the fourth ventricle 10) anterolateral and 11) posterior median sulci of the medulla 12) olivary zone 13) lateral medullary zone PONS MIDBRAIN MEDULLA
- 32. MIDBRAIN Anterior Mesencephalic Zone • Lesions involving the anterior midbrain can be accessed through a limited area on the cerebral peduncle bounded medially by the oculomotor tract and nerve and laterally by the corticospinal tract. • The entry point inside the interpeduncular cistern is limited superiorly by the posterior cerebral artery (PCA) and inferiorly by the main trunk of the superior cerebellar artery (SCA).
- 34. Lateral Mesencephalic Sulcus • The lateral mesencephalic sulcus extends downward in a concave fashion from the medial geniculate body to the pontomesencephalic sulcus. • The average total length of the sulcus was 9.6 mm (range 7.4–13.3 mm) with an average working-channel length of 8.0 mm.
- 35. Intercollicular Region • The most appropriate area for a small neurotomy has been described as the intercollicular region, because of its sparseness of fibers.
- 36. PONS Peritrigeminal Zone • The anterolateral surface of the pons has traditionally been considered a safe zone for entering the brainstem. • On the axial plane, a mean distance of 4.64 mm (range 3.8–5.6 mm) between CN V and the corticospinal tract, and a mean depth of dissection of 11.2 mm (range 9.5–13.1 mm) to the trigeminal nuclei.
- 37. Supratrigeminal Zone • Taking advantage of the posterolateral location of the middle cerebellar peduncle and the thick pontine transverse fibers, it is possible to carefully dissect along these fibers, medially or anteromedially, posterior to the trajectory of the corticospinal tract.
- 39. Lateral Pontine Zone • A safe corridor on the junction between the middle cerebellar peduncle and the pons and between the trigeminal and the facial-vestibulocochlear complex root entry zones.
- 40. Median Sulcus of the Fourth Ventricle • An approach through the midline, between the projection of the CN VI nuclei and the projection of the CN III nuclei on the midbrain surface. • Even the slightest lateral retraction may provoke extraocular movement disorders caused by damage to the medial longitudinal fascicle.
- 41. Supracollicular and Infracollicular Zones • Suprafacial triangle - caudally by the facial nerve, laterally by the cerebellar peduncles, and medially by the medial longitudinal fascicle. • Infrafacial triangle - striae medullaris caudally, the facial nerve laterally, and the medial longitudinal fascicle medially.
- 42. MEDULLA Anterolateral Sulcus • Just lateral to the pyramid, the rootlets of the hypoglossal nerve leave the brainstem on the anterolateral sulcus. • The short space between these rootlets and those of the C-1 nerve coincides with the decussation of the corticospinal tract. • A paramedian oblique dissection may avoid the corticospinal tract and address lesions of the anterior lower medullary region.
- 43. Posterior Median Sulcus • A neurotomy on the median sulcus provides a corridor near the center of the medulla. Lateral Medullary Zone “Inferior Cerebellar Peduncle Approach” • Safe entry zone for resection of dorsolateral medullary lesions. • Lesions were approached through the foramen of Luschka with an incision in the inferior cerebellar peduncle.
- 44. Olivary Zone • The olives are marked oval eminences on the anterolateral surface of the medulla, limited medially by the anterolateral sulcus and the pyramids and posteriorly by the posterolateral sulcus. • A safe depth of dissection via the olive, ranging from 4.7 to 6.9 mm, with a vertical length of 13.5 mm.
- 45. General Technique for Resection of well-encapsulated Lesions • Vertically open a pial or an ependymal brainstem surface, parallel to the fibers at the level of the safe-entry zone, using bayonet microforceps instead of a blade. • The opening of the forceps is used to stretch and displace fibers to allow the surgeon to reach the lesion. • After exposure of the lesion, use micropituitary forceps, dissectors, suction, and cautery to remove the lesion in a piecemeal fashion.
- 46. • In cases of cavernous malformations, the gliotic tissue surrounding the cavernous malformation and the developmental venous anomaly should be preserved. • After complete removal of the lesion, hemostasis is achieved using electrocautery on a low setting. • Alternatively, hemostatics may be placed into the resection cavity to assist with hemostasis but should be removed upon completion of the procedure